S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Mount Wilga High Level Language Test (Revised) (2006)Document78 paginiMount Wilga High Level Language Test (Revised) (2006)Speech & Language Therapy in Practice75% (8)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Sattler-Assessment of Children PDFDocument67 paginiSattler-Assessment of Children PDFTakashi Aoki100% (6)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Case Study 2Document2 paginiCase Study 2DUDUNG dudongÎncă nu există evaluări
- Talking Mats: Speech and Language Research in PracticeDocument4 paginiTalking Mats: Speech and Language Research in PracticeSpeech & Language Therapy in PracticeÎncă nu există evaluări
- The Big Five Personality Test - Truity MBA056 PDFDocument10 paginiThe Big Five Personality Test - Truity MBA056 PDFSaurav RathiÎncă nu există evaluări
- In Brief (Spring 11) Dementia and PhonologyDocument1 paginăIn Brief (Spring 11) Dementia and PhonologySpeech & Language Therapy in PracticeÎncă nu există evaluări
- Ylvisaker HandoutDocument20 paginiYlvisaker HandoutSpeech & Language Therapy in PracticeÎncă nu există evaluări
- A Practical FocusDocument2 paginiA Practical FocusSpeech & Language Therapy in PracticeÎncă nu există evaluări
- Test ResultDocument1 paginăTest ResultNicole AnahiÎncă nu există evaluări
- Mini Cog FormDocument2 paginiMini Cog FormAnonymous SVy8sOsvJDÎncă nu există evaluări
- Winning Ways (Spring 2008)Document1 paginăWinning Ways (Spring 2008)Speech & Language Therapy in PracticeÎncă nu există evaluări
- Turning On The SpotlightDocument6 paginiTurning On The SpotlightSpeech & Language Therapy in PracticeÎncă nu există evaluări
- Winning Ways (Winter 2007)Document1 paginăWinning Ways (Winter 2007)Speech & Language Therapy in PracticeÎncă nu există evaluări
- Imprints of The MindDocument5 paginiImprints of The MindSpeech & Language Therapy in PracticeÎncă nu există evaluări
- Here's One Sum 09 Storyteller, Friendship, That's HowDocument1 paginăHere's One Sum 09 Storyteller, Friendship, That's HowSpeech & Language Therapy in PracticeÎncă nu există evaluări
- Winning Ways (Autumn 2008)Document1 paginăWinning Ways (Autumn 2008)Speech & Language Therapy in PracticeÎncă nu există evaluări
- Here's One I Made Earlier (Spring 2008)Document1 paginăHere's One I Made Earlier (Spring 2008)Speech & Language Therapy in PracticeÎncă nu există evaluări
- Here's One SPR 09 Friendship ThemeDocument1 paginăHere's One SPR 09 Friendship ThemeSpeech & Language Therapy in PracticeÎncă nu există evaluări
- In Brief (Spring 09) Speed of SoundDocument1 paginăIn Brief (Spring 09) Speed of SoundSpeech & Language Therapy in PracticeÎncă nu există evaluări
- Winning Ways (Summer 2008)Document1 paginăWinning Ways (Summer 2008)Speech & Language Therapy in PracticeÎncă nu există evaluări
- In Brief and Critical Friends (Summer 09)Document1 paginăIn Brief and Critical Friends (Summer 09)Speech & Language Therapy in PracticeÎncă nu există evaluări
- In Brief and Here's One Autumn 10Document2 paginiIn Brief and Here's One Autumn 10Speech & Language Therapy in PracticeÎncă nu există evaluări
- Here's One Aut 09 Communication Tree, What On EarthDocument1 paginăHere's One Aut 09 Communication Tree, What On EarthSpeech & Language Therapy in PracticeÎncă nu există evaluări
- In Brief (Autumn 09) NQTs and Assessment ClinicsDocument1 paginăIn Brief (Autumn 09) NQTs and Assessment ClinicsSpeech & Language Therapy in PracticeÎncă nu există evaluări
- In Brief (Summer 10) TeenagersDocument1 paginăIn Brief (Summer 10) TeenagersSpeech & Language Therapy in PracticeÎncă nu există evaluări
- Here's One Spring 10 Dating ThemeDocument1 paginăHere's One Spring 10 Dating ThemeSpeech & Language Therapy in PracticeÎncă nu există evaluări
- In Brief (Spring 10) Acknowledgement, Accessibility, Direct TherapyDocument1 paginăIn Brief (Spring 10) Acknowledgement, Accessibility, Direct TherapySpeech & Language Therapy in PracticeÎncă nu există evaluări
- Here's One Winter 10Document1 paginăHere's One Winter 10Speech & Language Therapy in PracticeÎncă nu există evaluări
- In Brief (Winter 10) Stammering and Communication Therapy InternationalDocument2 paginiIn Brief (Winter 10) Stammering and Communication Therapy InternationalSpeech & Language Therapy in PracticeÎncă nu există evaluări
- Here's One Spring 11Document1 paginăHere's One Spring 11Speech & Language Therapy in PracticeÎncă nu există evaluări
- Here's One Summer 10Document1 paginăHere's One Summer 10Speech & Language Therapy in PracticeÎncă nu există evaluări
- Here's One I Made Earlier Summer 11Document1 paginăHere's One I Made Earlier Summer 11Speech & Language Therapy in PracticeÎncă nu există evaluări
- In Brief (Summer 11) AphasiaDocument1 paginăIn Brief (Summer 11) AphasiaSpeech & Language Therapy in PracticeÎncă nu există evaluări
- Boundary Issues (7) : Drawing The LineDocument1 paginăBoundary Issues (7) : Drawing The LineSpeech & Language Therapy in PracticeÎncă nu există evaluări
- Applying Choices and PossibilitiesDocument3 paginiApplying Choices and PossibilitiesSpeech & Language Therapy in PracticeÎncă nu există evaluări
- The Tight Tan Slacks of Dezso Ban - Size and Strength - Fred Koch and Tudor BompaDocument4 paginiThe Tight Tan Slacks of Dezso Ban - Size and Strength - Fred Koch and Tudor BompaCD KHUTIYALEÎncă nu există evaluări
- Bion and Primitive Mental States Trauma and The Symbiotic Link (Judy K. Eekhoff)Document159 paginiBion and Primitive Mental States Trauma and The Symbiotic Link (Judy K. Eekhoff)noseyatiaÎncă nu există evaluări
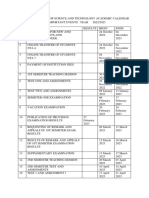
- Almanac 2022-2023Document2 paginiAlmanac 2022-2023khatib mtumweniÎncă nu există evaluări
- Barangay Council For The Protection of ChildrenDocument6 paginiBarangay Council For The Protection of ChildrenGem BesandeÎncă nu există evaluări
- 3 - 1 Intro 2 General Safety PracticesDocument3 pagini3 - 1 Intro 2 General Safety PracticesKevin Sánchez RodríguezÎncă nu există evaluări
- Operant Conditioning: - B F Skinner (1948)Document12 paginiOperant Conditioning: - B F Skinner (1948)AmanÎncă nu există evaluări
- OSH ProgrammingDocument29 paginiOSH Programmingmarlyn madambaÎncă nu există evaluări
- The Newborn ExaminationDocument132 paginiThe Newborn ExaminationdevilstÎncă nu există evaluări
- MANIADocument1 paginăMANIALillabinÎncă nu există evaluări
- Assessment of Health RisksDocument27 paginiAssessment of Health RisksMohamed GHAFFARÎncă nu există evaluări
- Module 3 FP Client AssessmentDocument54 paginiModule 3 FP Client AssessmentJhunna TalanganÎncă nu există evaluări
- Toolbox Talks - Near Miss ReportingDocument1 paginăToolbox Talks - Near Miss ReportinganaÎncă nu există evaluări
- HousekeepingDocument18 paginiHousekeepingমুসফেকআহমেদনাহিদÎncă nu există evaluări
- National Service Training Program Service Learning Program: Help The VulnerableDocument11 paginiNational Service Training Program Service Learning Program: Help The VulnerableBrunhild BangayanÎncă nu există evaluări
- Doctor'S Order and Progress NotesDocument3 paginiDoctor'S Order and Progress NotesDienizs LabiniÎncă nu există evaluări
- Template Traffic Light MatrixDocument1 paginăTemplate Traffic Light MatrixDivalita100% (1)
- Classroom Activity CHCDIS003Document4 paginiClassroom Activity CHCDIS003Sonam GurungÎncă nu există evaluări
- Blue Eyes Brown Eyes Nov 10 2021Document31 paginiBlue Eyes Brown Eyes Nov 10 2021Emmy S.U.Încă nu există evaluări
- Critical Analysis REBTDocument4 paginiCritical Analysis REBTMehar KhanÎncă nu există evaluări
- Detail of Rajiv Gandhi Jeevandayee Arogya Yojana MaharashtraDocument180 paginiDetail of Rajiv Gandhi Jeevandayee Arogya Yojana MaharashtraBrandon Bell100% (1)
- Banco de Preguntas ReabilitacionDocument19 paginiBanco de Preguntas ReabilitacionVanessa AlcantaraÎncă nu există evaluări
- Ramos Persuasive-Essay 3rdDocument3 paginiRamos Persuasive-Essay 3rdMa. Cassandra A. RamosÎncă nu există evaluări
- Cultural ListDocument7 paginiCultural ListTilakÎncă nu există evaluări
- Postnatal DepressionDocument36 paginiPostnatal DepressionMariam Matchavariani100% (1)
- Zoono Fact Sheet 53 - Comparison Between Dettol Hand Sanitiser and GermF...Document2 paginiZoono Fact Sheet 53 - Comparison Between Dettol Hand Sanitiser and GermF...Eileen Le RouxÎncă nu există evaluări