S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Face PresentationDocument6 paginiFace PresentationNishaThakuriÎncă nu există evaluări
- Pain ADocument19 paginiPain Akcc2012Încă nu există evaluări
- Post-Operative Abdominal Infections: Epidemiology, Operational Definitions, and OutcomesDocument10 paginiPost-Operative Abdominal Infections: Epidemiology, Operational Definitions, and OutcomesJared CossioÎncă nu există evaluări
- Pediatric Neuropsychology Case Studies PDFDocument358 paginiPediatric Neuropsychology Case Studies PDFGabriela Hernandez100% (1)
- Binge EatingDocument18 paginiBinge EatingIuliana IgnatÎncă nu există evaluări
- Cholelithiasis SampleDocument77 paginiCholelithiasis Samplekrischamcute67% (3)
- Prescription - Apollo 2471688806157843Document2 paginiPrescription - Apollo 2471688806157843shahidliftsÎncă nu există evaluări
- Phytochemical Screening and Extraction A ReviewDocument9 paginiPhytochemical Screening and Extraction A Reviewsaivasya50% (2)
- Lesser Metatarsal Osteotomy Complications: Lowell S. Weil and Erin E. KleinDocument9 paginiLesser Metatarsal Osteotomy Complications: Lowell S. Weil and Erin E. KleinAntonio FloresÎncă nu există evaluări
- Windy WigaDocument2 paginiWindy WigaWindy wigaÎncă nu există evaluări
- 2016 S 0042 108641 PDFDocument29 pagini2016 S 0042 108641 PDFMadalina StoicescuÎncă nu există evaluări
- Varma Varmam Marma Book Full Color in English - VKRC Vol 2 Book S Ramesh Babu - Free PDF DownloadDocument14 paginiVarma Varmam Marma Book Full Color in English - VKRC Vol 2 Book S Ramesh Babu - Free PDF DownloadS Ramesh BabuÎncă nu există evaluări
- 09022016att ComplaintDocument25 pagini09022016att Complaintsarah_larimerÎncă nu există evaluări
- Mic Eales A Visual Enquiry Into SuicideDocument4 paginiMic Eales A Visual Enquiry Into Suicidemaribolla8015Încă nu există evaluări
- Vertigo MeniereDocument5 paginiVertigo MeniereHamba AllahÎncă nu există evaluări
- ABR Workout GuideDocument13 paginiABR Workout GuideGJONES80100% (1)
- 200 Terms & Definition From Pharmacology. WatermarkedDocument17 pagini200 Terms & Definition From Pharmacology. Watermarkedsuresh adgaonkar100% (1)
- HbA1c - I Chrome DuoDocument3 paginiHbA1c - I Chrome DuoAnnisa Chaerani100% (1)
- DolcetDocument3 paginiDolcetConn_Casipe_8158100% (4)
- Theraputic UltrasoundDocument64 paginiTheraputic UltrasoundRoshni KhanÎncă nu există evaluări
- Reiki 1Document19 paginiReiki 1api-246890707Încă nu există evaluări
- Sistem Pelaporan Dan Pembelajaran Keselamatan Pasien RS Arjaty 2022Document13 paginiSistem Pelaporan Dan Pembelajaran Keselamatan Pasien RS Arjaty 2022vera kusunyadewiÎncă nu există evaluări
- Tanggal Rujuk BalnamaDocument7 paginiTanggal Rujuk BalnamapkmjemursariÎncă nu există evaluări
- Transfusion Reaction PDFDocument1 paginăTransfusion Reaction PDFKah Man GohÎncă nu există evaluări
- Drug Descrubrimiento de FarmacosDocument302 paginiDrug Descrubrimiento de FarmacosdavidÎncă nu există evaluări
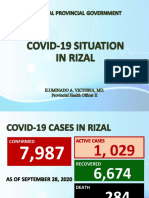
- Covid19 Situation in RizalDocument23 paginiCovid19 Situation in RizalToni Quitalig GamezÎncă nu există evaluări
- Skin Care Plan: Nu Derm Protocol ForDocument7 paginiSkin Care Plan: Nu Derm Protocol ForsheilaÎncă nu există evaluări
- Principle of Laser Application in Medicine & LASER SAFETY5Document62 paginiPrinciple of Laser Application in Medicine & LASER SAFETY5melisandrianaÎncă nu există evaluări
- Basic Priciples of Heart SurgeryDocument6 paginiBasic Priciples of Heart SurgeryprofarmahÎncă nu există evaluări
- Parkinsons Presentation Case StudyDocument33 paginiParkinsons Presentation Case Studyapi-287759747Încă nu există evaluări