S-ar putea să vă placă și
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Psychoanalisis and PaediatricsDocument264 paginiPsychoanalisis and PaediatricsBlackKÎncă nu există evaluări
- Icu PDFDocument49 paginiIcu PDFVidya GopiÎncă nu există evaluări
- The Life Inside - TreatmentDocument7 paginiThe Life Inside - TreatmentTakashi DoscherÎncă nu există evaluări
- KyphiDocument4 paginiKyphiPhlegisÎncă nu există evaluări
- Restorative Management of The Worn Dentition Pt1Document6 paginiRestorative Management of The Worn Dentition Pt1Sherif ReffatÎncă nu există evaluări
- Space LossDocument5 paginiSpace LossAsma NawazÎncă nu există evaluări
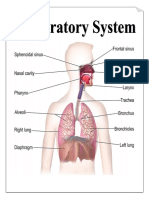
- Parts & Function of Respiratory SystemDocument4 paginiParts & Function of Respiratory SystemLucille Ballares83% (6)
- H3 A5Document52 paginiH3 A5Jenny RosaliÎncă nu există evaluări
- Presentation GoodridgeDocument103 paginiPresentation GoodridgeAlexandra Papp67% (3)
- DENTIST ReferencesDocument3 paginiDENTIST ReferencesAsma NawazÎncă nu există evaluări
- Dr. Shubhangi Mhaske - OSFDocument6 paginiDr. Shubhangi Mhaske - OSFAsma NawazÎncă nu există evaluări
- Dental Specialty SOPDocument1 paginăDental Specialty SOPAsma NawazÎncă nu există evaluări
- RetDocument1 paginăRetAsma NawazÎncă nu există evaluări
- PJMS MS 145 SPK Vol 9 No 2 2012-8Document7 paginiPJMS MS 145 SPK Vol 9 No 2 2012-8Asma NawazÎncă nu există evaluări
- 3 2 6Document7 pagini3 2 6Asma NawazÎncă nu există evaluări
- 3 2 6Document7 pagini3 2 6Asma NawazÎncă nu există evaluări
- Archive of SID: Oral Submucous Fibrosis in A 15-Year-Old Boy: The First Case Report in IranDocument5 paginiArchive of SID: Oral Submucous Fibrosis in A 15-Year-Old Boy: The First Case Report in IranAsma NawazÎncă nu există evaluări
- Oral Submucous FIbrosisDocument13 paginiOral Submucous FIbrosisAsma NawazÎncă nu există evaluări
- Oral Submucous Fibrosis, Pre MalignantDocument38 paginiOral Submucous Fibrosis, Pre MalignantHaris Mehmood100% (3)
- Bulimia NervosaDocument4 paginiBulimia NervosaAsma NawazÎncă nu există evaluări
- Tooth LossDocument3 paginiTooth LossAsma NawazÎncă nu există evaluări
- AttritionDocument7 paginiAttritionAsma NawazÎncă nu există evaluări
- Non CariousDocument19 paginiNon CariousAsma NawazÎncă nu există evaluări
- How To Overcome FailedDocument14 paginiHow To Overcome FailedAsma NawazÎncă nu există evaluări
- Acute and Chronic Gastritis Due To Helicobacter PyloriDocument8 paginiAcute and Chronic Gastritis Due To Helicobacter PyloriCarla HolandÎncă nu există evaluări
- Bullying and Ostracism Experiences in Children - JDBPDocument9 paginiBullying and Ostracism Experiences in Children - JDBPAndreea Gligor100% (1)
- UHC Vision Plan SummaryDocument2 paginiUHC Vision Plan SummaryJanet Zimmerman McNicholÎncă nu există evaluări
- Hemorrhagic Disease of The NewbornDocument2 paginiHemorrhagic Disease of The NewbornsucirahmiiiiiiÎncă nu există evaluări
- Paederus Dermatitis An Outbreak On A Medical Mission AmazonDocument3 paginiPaederus Dermatitis An Outbreak On A Medical Mission AmazonrrrawÎncă nu există evaluări
- Ultrafiltration Failure in Peritoneal Dialysis: A Pathophysiologic ApproachDocument4 paginiUltrafiltration Failure in Peritoneal Dialysis: A Pathophysiologic ApproachAn-Nisa Khoirun UmmiÎncă nu există evaluări
- Curriculum Vitae Andreas Dietz MD PHDDocument2 paginiCurriculum Vitae Andreas Dietz MD PHDalexandru_andreaÎncă nu există evaluări
- NSO7Document3 paginiNSO7Edmund RufinoÎncă nu există evaluări
- Charateristics of NewbornDocument3 paginiCharateristics of NewbornRagupathyRamanjuluÎncă nu există evaluări
- Anatomy of The KidneyDocument13 paginiAnatomy of The KidneyChristi NaldoÎncă nu există evaluări
- Does Platform Switching Really Prevent Crestal Bone Loss Around Implants?Document46 paginiDoes Platform Switching Really Prevent Crestal Bone Loss Around Implants?manujohnsÎncă nu există evaluări
- Randomized, Placebo-Controlled Trial of Xyloglucan and Gelose For The Treatment of Acute Diarrhea in ChildrenDocument8 paginiRandomized, Placebo-Controlled Trial of Xyloglucan and Gelose For The Treatment of Acute Diarrhea in ChildrenvalenciaÎncă nu există evaluări
- Winona Health - Healthy Connections Spring 2007Document16 paginiWinona Health - Healthy Connections Spring 2007winonahealthÎncă nu există evaluări
- Helens ResumeDocument1 paginăHelens Resumeapi-514514226Încă nu există evaluări
- Ethiopian Hospitals Servcie Transformation Guideline Volume 2 PDFDocument437 paginiEthiopian Hospitals Servcie Transformation Guideline Volume 2 PDFAREGAWI WELDUÎncă nu există evaluări
- Perforated Peptic Ulcer DiseaseDocument9 paginiPerforated Peptic Ulcer DiseaseMade Oka HeryanaÎncă nu există evaluări
- Daftar Pustaka KBDocument3 paginiDaftar Pustaka KBYogi OktiandiÎncă nu există evaluări
- Efficacy of Homoeopathy in Treatment of Sarcoidosis 100 CasesDocument39 paginiEfficacy of Homoeopathy in Treatment of Sarcoidosis 100 CasesDr. Rajneesh Kumar Sharma MD HomÎncă nu există evaluări
- CV NursingDocument4 paginiCV Nursingapi-355295086Încă nu există evaluări
- Paracetamol A Review of Three Routes of AdministrationDocument3 paginiParacetamol A Review of Three Routes of AdministrationMohd MiqdamÎncă nu există evaluări
- Best Docs - Aug 09Document18 paginiBest Docs - Aug 09AY Magazine100% (2)
- Book 1Document6 paginiBook 1Kieth Garcia DariaÎncă nu există evaluări
- Porcelain Fused To Metal CrownsDocument5 paginiPorcelain Fused To Metal CrownsCitra Dwi PrastiwieÎncă nu există evaluări