S-ar putea să vă placă și
- Oral Medicine & Pathology from A-ZDe la EverandOral Medicine & Pathology from A-ZEvaluare: 5 din 5 stele5/5 (9)
- QDT 2012 Prov PDFDocument14 paginiQDT 2012 Prov PDFVania Sánchez100% (2)
- Minimally Invasive Treatment of InitialDocument15 paginiMinimally Invasive Treatment of Initialnoskov100% (2)
- 34 3 329 Vojvodic enDocument2 pagini34 3 329 Vojvodic enDiana BărbulescuÎncă nu există evaluări
- 322 1403 1 PB PDFDocument2 pagini322 1403 1 PB PDFAdityaÎncă nu există evaluări
- Oral Sub-Mucous FibrosisDocument2 paginiOral Sub-Mucous FibrosisShreyans DamadeÎncă nu există evaluări
- An Integrated Treatment Approach: A Case Report For Dentinogenesis Imperfecta Type IIDocument4 paginiAn Integrated Treatment Approach: A Case Report For Dentinogenesis Imperfecta Type IIpritasyaÎncă nu există evaluări
- OsmfDocument7 paginiOsmfRhea MalikÎncă nu există evaluări
- 01 A Method For Positioning The Premaxilla During Impression MakingDocument4 pagini01 A Method For Positioning The Premaxilla During Impression MakingalonsoÎncă nu există evaluări
- Gigi Tiruan GasketDocument5 paginiGigi Tiruan GasketGus BasyaÎncă nu există evaluări
- Case ReportDocument10 paginiCase ReportwidhariyaniÎncă nu există evaluări
- Three-Dimensional Soft Tissue Evaluation After Rapid Maxillary Expansion and Mandibular Midline Distraction OsteogenesisDocument7 paginiThree-Dimensional Soft Tissue Evaluation After Rapid Maxillary Expansion and Mandibular Midline Distraction OsteogenesisayisÎncă nu există evaluări
- Pin-Retained Restoration With Resin Bonded Composite of A Badly Broken ToothDocument3 paginiPin-Retained Restoration With Resin Bonded Composite of A Badly Broken ToothIOSRjournalÎncă nu există evaluări
- Indirect Veneer Treatment of Anterior Maxillary Teeth With Enamel HypoplasiaDocument5 paginiIndirect Veneer Treatment of Anterior Maxillary Teeth With Enamel Hypoplasiaamalia rieska mauliddyaÎncă nu există evaluări
- Prosthodontic Management of Severely ResorbedDocument2 paginiProsthodontic Management of Severely ResorbedAamir BugtiÎncă nu există evaluări
- Restoring Function and Esthetics in 2 Patients With Amelogenesis Imperfecta: Case ReportDocument0 paginiRestoring Function and Esthetics in 2 Patients With Amelogenesis Imperfecta: Case ReportYulinda PrimilisaÎncă nu există evaluări
- Tooth WearDocument11 paginiTooth WearNaji Z. ArandiÎncă nu există evaluări
- Diastema Closure With Direct Composite Architectural Gingival Contouring.20150306122816Document6 paginiDiastema Closure With Direct Composite Architectural Gingival Contouring.20150306122816Rossye MpfÎncă nu există evaluări
- Full Mouth Rehabilitation of The Patient With Severly Worn Out Dentition A Case Report.Document5 paginiFull Mouth Rehabilitation of The Patient With Severly Worn Out Dentition A Case Report.sivak_198100% (1)
- Patient Selection in Lingual OrthodonticsDocument8 paginiPatient Selection in Lingual OrthodonticsSreenivasa Krishna ChaitanyaÎncă nu există evaluări
- Fabrication of Conventional Complete Dentures For A Left Segmental MandibulectomyDocument4 paginiFabrication of Conventional Complete Dentures For A Left Segmental MandibulectomyIndrani DasÎncă nu există evaluări
- C@rllas-Shivani Parmar-Ankita SharmaDocument5 paginiC@rllas-Shivani Parmar-Ankita SharmaJony OcañaÎncă nu există evaluări
- Pediatric ProsthodonticsDocument84 paginiPediatric Prosthodonticsnihu100% (2)
- Aldrigui 2011Document5 paginiAldrigui 2011Javier Farias VeraÎncă nu există evaluări
- Gingival Mask 2013Document3 paginiGingival Mask 2013annysaÎncă nu există evaluări
- Immediate Complete DenturesDocument74 paginiImmediate Complete DenturesPuneet Pandher100% (1)
- Completedenture Theory and PracticeDocument1.233 paginiCompletedenture Theory and PracticeMostafa Fayad100% (7)
- An Alternative Solution For A Complex Prosthodontic Problem: A Modified Andrews Fixed Dental ProsthesisDocument5 paginiAn Alternative Solution For A Complex Prosthodontic Problem: A Modified Andrews Fixed Dental ProsthesisDragos CiongaruÎncă nu există evaluări
- Additive Contour of Porcelain Veneers A Key Element in Enamel PreservationDocument13 paginiAdditive Contour of Porcelain Veneers A Key Element in Enamel PreservationPablo BenitezÎncă nu există evaluări
- IRA Klein,: Mmedmte Denture ServiceDocument11 paginiIRA Klein,: Mmedmte Denture ServiceClaudia AngÎncă nu există evaluări
- Overlay DentureDocument5 paginiOverlay DentureAmar BhochhibhoyaÎncă nu există evaluări
- OverdentureDocument76 paginiOverdentureRaj Sha80% (5)
- 35 2 281 Kraljevic enDocument5 pagini35 2 281 Kraljevic ensss2013Încă nu există evaluări
- Shortened Dental ArchDocument5 paginiShortened Dental Archsarah wilderÎncă nu există evaluări
- The Socket-Shield Technique To Support The Buccofacial Tissues at Immediate Implant Placement PDFDocument7 paginiThe Socket-Shield Technique To Support The Buccofacial Tissues at Immediate Implant Placement PDFAhmed Mohammed Saaduddin SapriÎncă nu există evaluări
- Esthetic Closure of Diastema by Porcelain Laminate Veneers: A Case ReportDocument4 paginiEsthetic Closure of Diastema by Porcelain Laminate Veneers: A Case ReportVirma PutraÎncă nu există evaluări
- DeninvaginatusDocument7 paginiDeninvaginatusScorpioster KikiÎncă nu există evaluări
- Ribbond For Treatment of Complicated Crown Fractures: Report of 3 CasesDocument4 paginiRibbond For Treatment of Complicated Crown Fractures: Report of 3 CasesAmmyÎncă nu există evaluări
- ArticleDocument4 paginiArticleDrRahul Puri GoswamiÎncă nu există evaluări
- Managing Discoloured Non-Vital Teeth: The Inside/Outside Bleaching TechniqueDocument8 paginiManaging Discoloured Non-Vital Teeth: The Inside/Outside Bleaching TechniqueJesus Manuel Lopez VidalÎncă nu există evaluări
- Interesting Eruption of 4 Teeth Associated With A Large Dentigerous Cyst in Mandible by Only MarsupializationDocument3 paginiInteresting Eruption of 4 Teeth Associated With A Large Dentigerous Cyst in Mandible by Only MarsupializationAnupama NagrajÎncă nu există evaluări
- 3Document4 pagini3Goutham SunilÎncă nu există evaluări
- R1a in Vivo Study of Use of Bioceramic MaterialDocument4 paginiR1a in Vivo Study of Use of Bioceramic MaterialIoana GrigorasÎncă nu există evaluări
- Management of Anterior Dental Crossbite With Removable AppliancesDocument4 paginiManagement of Anterior Dental Crossbite With Removable AppliancesSurya WijayaÎncă nu există evaluări
- Natural Tooth Pontic in Periodontally Compromised ToothDocument5 paginiNatural Tooth Pontic in Periodontally Compromised ToothAmar BhochhibhoyaÎncă nu există evaluări
- Esthetic Zone Root Coverage With Lateral Pedicle Flap - A CaseDocument5 paginiEsthetic Zone Root Coverage With Lateral Pedicle Flap - A CaseHiroj BagdeÎncă nu există evaluări
- Compomer CrownDocument2 paginiCompomer CrownIndah SimamoraÎncă nu există evaluări
- Adhesive Restorations Centric RelationDocument14 paginiAdhesive Restorations Centric RelationIlse100% (1)
- 6-Year-Follo Up. 3 Steps Techniques. Francesca Valati-1 PDFDocument25 pagini6-Year-Follo Up. 3 Steps Techniques. Francesca Valati-1 PDFAdriana CoronadoÎncă nu există evaluări
- Direct Laminate Veneers With Resin Composites: Two Case Reports With Five-Year Follow-UpsDocument7 paginiDirect Laminate Veneers With Resin Composites: Two Case Reports With Five-Year Follow-UpsBarbulescu Anca DianaÎncă nu există evaluări
- FMR of Worn Out DentititonDocument6 paginiFMR of Worn Out Dentititonrayavarapu sunilÎncă nu există evaluări
- PEAK Restoration of The Endodontically Treated ToothDocument20 paginiPEAK Restoration of The Endodontically Treated Toothlishenwong100% (1)
- Orthodontic and Orthopedic Treatment of A Patient With Incontinentia PigmentiDocument6 paginiOrthodontic and Orthopedic Treatment of A Patient With Incontinentia PigmentiGisselaMaldonadoÎncă nu există evaluări
- Mouth Preperation RPDDocument14 paginiMouth Preperation RPDSadishÎncă nu există evaluări
- Case Report Massive Radicular Cyst in The Maxillary Sinus As A Result of Deciduous Molar Tooth Pulp NecrosisDocument5 paginiCase Report Massive Radicular Cyst in The Maxillary Sinus As A Result of Deciduous Molar Tooth Pulp NecrosisSarah Ariefah SantriÎncă nu există evaluări
- Neutral Zone and Oral Submucous Fibrosis: Ase EportDocument4 paginiNeutral Zone and Oral Submucous Fibrosis: Ase EportAmit SadhwaniÎncă nu există evaluări
- Asds 02 0215Document3 paginiAsds 02 02156mf9jf6h99Încă nu există evaluări
- Franchini Judo Active Recovery EJAP 2009Document7 paginiFranchini Judo Active Recovery EJAP 2009Buzatu IonelÎncă nu există evaluări
- Specificatii Tractoare Seria 5Document2 paginiSpecificatii Tractoare Seria 5David Paul ClaudiuÎncă nu există evaluări
- J 1600-0765 2010 01335 XDocument5 paginiJ 1600-0765 2010 01335 XBuzatu IonelÎncă nu există evaluări
- Cls II KenDocument10 paginiCls II KenBuzatu IonelÎncă nu există evaluări
- Unconventional Prosthodontics: Post, Core and Crown TechniqueDocument5 paginiUnconventional Prosthodontics: Post, Core and Crown TechniqueBuzatu IonelÎncă nu există evaluări
- Cls I KenDocument13 paginiCls I KenBuzatu IonelÎncă nu există evaluări
- 2010 Oral Health Systems in EuropeDocument28 pagini2010 Oral Health Systems in EuropeBuzatu IonelÎncă nu există evaluări
- A New Design For Anterior Fixed Partial Denture, Combining Facial Porcelain and Lingual Metal PTU Type IIDocument5 paginiA New Design For Anterior Fixed Partial Denture, Combining Facial Porcelain and Lingual Metal PTU Type IIBuzatu IonelÎncă nu există evaluări
- 99 Ppav 11 N 1 P 95Document13 pagini99 Ppav 11 N 1 P 95Buzatu IonelÎncă nu există evaluări
- Ijo 25 239Document6 paginiIjo 25 239Buzatu IonelÎncă nu există evaluări
- CancerDocument10 paginiCancerBuzatu IonelÎncă nu există evaluări
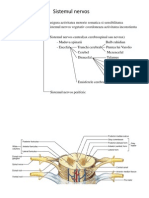
- Maduva Spinarii. Trunchiul Cerebral. CerebelDocument35 paginiMaduva Spinarii. Trunchiul Cerebral. CerebelI.m. DanielÎncă nu există evaluări
- Jap 4 109Document7 paginiJap 4 109Buzatu IonelÎncă nu există evaluări
- Regression MethodsDocument7 paginiRegression MethodsBuzatu IonelÎncă nu există evaluări
- Maduva Spinarii. Trunchiul Cerebral. CerebelDocument35 paginiMaduva Spinarii. Trunchiul Cerebral. CerebelI.m. DanielÎncă nu există evaluări
- Jap 4 97Document6 paginiJap 4 97Buzatu IonelÎncă nu există evaluări
- 10.1007 - s13191 011 0046 0Document7 pagini10.1007 - s13191 011 0046 0Rivemi GusyantiÎncă nu există evaluări
- Maxillofacial Rehabilitation of Nasal Defect With Nasal Prosthesis Using Donor Method: A Case ReportDocument4 paginiMaxillofacial Rehabilitation of Nasal Defect With Nasal Prosthesis Using Donor Method: A Case ReportAndra AgheorghieseiÎncă nu există evaluări
- Eview Rticle: Journal of Advanced Medical and Dental Sciences ResearchDocument3 paginiEview Rticle: Journal of Advanced Medical and Dental Sciences ResearchSwathiLingannagariÎncă nu există evaluări
- 11 - Soft Tissue Waxup and Mock-Up and Key Factors inDocument15 pagini11 - Soft Tissue Waxup and Mock-Up and Key Factors inPablo BenitezÎncă nu există evaluări
- Lyons Et Al-2017-Periodontology 2000Document4 paginiLyons Et Al-2017-Periodontology 2000Julio César PlataÎncă nu există evaluări
- IPlus BrochureDocument42 paginiIPlus BrochureZain Ayub100% (1)
- Reconstructive Aesthetic Implant SurgeryDocument156 paginiReconstructive Aesthetic Implant SurgeryOanaroxana Varsa100% (1)
- 5 Exclusive Techniques - RESIDUAL RIDGE RESORPTION - ExtoothDocument18 pagini5 Exclusive Techniques - RESIDUAL RIDGE RESORPTION - ExtoothHugo MoralesÎncă nu există evaluări
- Full Prosthetic BookDocument132 paginiFull Prosthetic BookJoseEspan100% (1)
- Zirconia in Dental Prosthetics: A Literature ReviewDocument9 paginiZirconia in Dental Prosthetics: A Literature ReviewSchuster StephanÎncă nu există evaluări
- DMFR 20220335Document22 paginiDMFR 20220335Albert CamusÎncă nu există evaluări
- Evaluation of Different EstheticDocument8 paginiEvaluation of Different EstheticSebastián BernalÎncă nu există evaluări
- Panoramic X RayDocument15 paginiPanoramic X Raymostafa khÎncă nu există evaluări
- 01-Hypro-Oss Clinical Assessment 2012 enDocument14 pagini01-Hypro-Oss Clinical Assessment 2012 enPaulus LagadanÎncă nu există evaluări
- Contribution of 3D Printing For The Surgical Management of Jaws Cysts and Benign Tumors: A Systematic Review of The LiteratureDocument9 paginiContribution of 3D Printing For The Surgical Management of Jaws Cysts and Benign Tumors: A Systematic Review of The LiteratureEsteban FernandezÎncă nu există evaluări
- Assessment of Level of Satisfaction and Problems in Patients Treated With Fixed Partial Denture in Alkharj City (Kingdom of Saudi Arabia)Document6 paginiAssessment of Level of Satisfaction and Problems in Patients Treated With Fixed Partial Denture in Alkharj City (Kingdom of Saudi Arabia)Mihaela VasiliuÎncă nu există evaluări
- Lesson - 1-Dental Prosthetics and DentistryDocument35 paginiLesson - 1-Dental Prosthetics and DentistryDuncan MakÎncă nu există evaluări
- Screw Versus Cement New DesignDocument3 paginiScrew Versus Cement New Designharshita parasharÎncă nu există evaluări
- Proyecto Final Ángela P. FierroDocument39 paginiProyecto Final Ángela P. Fierro9bh4spchgsÎncă nu există evaluări
- Dentis - OneQ CatalogueDocument52 paginiDentis - OneQ CatalogueAnonymous GMHivr50% (2)
- Considerations For Orthognathic Surgery During Growth, Part 1 - Mandibular DeformitiesDocument7 paginiConsiderations For Orthognathic Surgery During Growth, Part 1 - Mandibular DeformitiesLeonardo LamimÎncă nu există evaluări
- Review Article: Guided Bone Regeneration: A Literature ReviewDocument16 paginiReview Article: Guided Bone Regeneration: A Literature ReviewGonçalo Gomes SanchesÎncă nu există evaluări
- Cat Prod Zhermack 08 EngDocument145 paginiCat Prod Zhermack 08 EngramukumarÎncă nu există evaluări
- JADA 2012 Balevi 1011 2Document3 paginiJADA 2012 Balevi 1011 2Linda RodriguezÎncă nu există evaluări
- CDE Course 2019Document19 paginiCDE Course 2019Ellen HungÎncă nu există evaluări
- Radiographic Evaluation of Crestal Bone Loss For Bar Retainedimplant Overdenture Supported by Four Implants Versus All On 4 Screw Retained ProsthesisDocument8 paginiRadiographic Evaluation of Crestal Bone Loss For Bar Retainedimplant Overdenture Supported by Four Implants Versus All On 4 Screw Retained ProsthesisIJAR JOURNALÎncă nu există evaluări
- 3m Espe Soft Monophase Tds IntDocument12 pagini3m Espe Soft Monophase Tds IntjaneÎncă nu există evaluări
- Implantarmamentarium 170902170115Document99 paginiImplantarmamentarium 170902170115Recep Vatansever0% (1)
- My First Tooth in An Hour CaseDocument35 paginiMy First Tooth in An Hour CaseRacovitanCÎncă nu există evaluări
- Indianjhealthsci16160-4648441 125444Document7 paginiIndianjhealthsci16160-4648441 125444Akhil DeshpandeÎncă nu există evaluări
- Curriculum VitaeDocument3 paginiCurriculum VitaeDental ImplantsÎncă nu există evaluări