S-ar putea să vă placă și
- Problem-based Approach to Gastroenterology and HepatologyDe la EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisÎncă nu există evaluări
- Antihyperglycemic Agents Comparison Chart PDFDocument9 paginiAntihyperglycemic Agents Comparison Chart PDFconcoz100% (1)
- Antihyperglycemic Agents Comparison ChartDocument9 paginiAntihyperglycemic Agents Comparison ChartBonnieÎncă nu există evaluări
- Abx FinalDocument3 paginiAbx Finalyanks1120Încă nu există evaluări
- How Do I Diagnose The Cause of A Cough of Less Than 3 Weeks' Duration?Document14 paginiHow Do I Diagnose The Cause of A Cough of Less Than 3 Weeks' Duration?Sudhir TyagiÎncă nu există evaluări
- PA 514 Intro To Infectious Disease SyllabusDocument11 paginiPA 514 Intro To Infectious Disease Syllabuslu100% (1)
- 10 - Infectious Diseases (9700 AS Biology)Document33 pagini10 - Infectious Diseases (9700 AS Biology)ho100% (1)
- Drug Toxicity and PoisoningDocument12 paginiDrug Toxicity and PoisoningPAULA MARIE MERCADO LLIDOÎncă nu există evaluări
- Medical Case 1: Language Centre of Malahayati University at 2010Document16 paginiMedical Case 1: Language Centre of Malahayati University at 2010putri1114Încă nu există evaluări
- Drug AllergyDocument61 paginiDrug Allergyadysti100% (1)
- 06.2 Inborn Error of Metabolism - Iii B - Trans PDFDocument10 pagini06.2 Inborn Error of Metabolism - Iii B - Trans PDFAshim AbhiÎncă nu există evaluări
- Finals PHARMACOTHERAPHY OF DIABETES MELLITUS 2017Document8 paginiFinals PHARMACOTHERAPHY OF DIABETES MELLITUS 2017Sheryl Layne Lao-SebrioÎncă nu există evaluări
- Assignment 2.1soap 1Document5 paginiAssignment 2.1soap 1Anonymous mX5wWmGÎncă nu există evaluări
- Article - Medical ErrorsDocument4 paginiArticle - Medical ErrorsDavid S. ChouÎncă nu există evaluări
- Mock Record B-1-2-Well Child VisitsDocument4 paginiMock Record B-1-2-Well Child VisitsaelteeÎncă nu există evaluări
- Antiarrhythmic Drugs: More To Inactivated Na Channels Arrhythmias During Myocardial Ischaemia or Due To DigoxinDocument3 paginiAntiarrhythmic Drugs: More To Inactivated Na Channels Arrhythmias During Myocardial Ischaemia or Due To DigoxinChia Yin NgÎncă nu există evaluări
- Medicine1 Grand PE ScriptDocument10 paginiMedicine1 Grand PE ScriptCarmeline Santi BeronillaÎncă nu există evaluări
- SOAP Note Example 32 Weeks OB CheckDocument4 paginiSOAP Note Example 32 Weeks OB CheckG. Crusor-PriceÎncă nu există evaluări
- 2018 Fall Geriatrics SyllabusDocument41 pagini2018 Fall Geriatrics SyllabusSen SioÎncă nu există evaluări
- Chapter 13. Heartburn and DyspepsiaDocument22 paginiChapter 13. Heartburn and DyspepsiaMonica CiorneiÎncă nu există evaluări
- H&P SampleDocument3 paginiH&P Samplelindsay_weiss_6Încă nu există evaluări
- Mu 002Document10 paginiMu 002chandanÎncă nu există evaluări
- 08&09 Oral Hypoglycemics-Level 11Document48 pagini08&09 Oral Hypoglycemics-Level 11Usman Ali AkbarÎncă nu există evaluări
- Mood Disorders: Advanced Practice Education AssociatesDocument11 paginiMood Disorders: Advanced Practice Education AssociatesAndrea100% (1)
- NSG6435 Soap3Document6 paginiNSG6435 Soap3Hephzibah BeulahÎncă nu există evaluări
- Classification of The Epilepsies: Purpose: For Clinical DiagnosisDocument25 paginiClassification of The Epilepsies: Purpose: For Clinical Diagnosisayu rifqiÎncă nu există evaluări
- Paracetamol PDFDocument49 paginiParacetamol PDFEhb90210Încă nu există evaluări
- Micro Chart #3 - Italics OnlyDocument27 paginiMicro Chart #3 - Italics Onlyapi-26938624100% (1)
- Rashes in Children by Dr. Muhammad - RashidDocument43 paginiRashes in Children by Dr. Muhammad - RashidAli DkaliÎncă nu există evaluări
- Asthma (For RACP Exams)Document18 paginiAsthma (For RACP Exams)Sam HuntÎncă nu există evaluări
- Hereditary HemochromatosisDocument6 paginiHereditary HemochromatosisVijeyachandhar DorairajÎncă nu există evaluări
- Introduction and Overview of Community Health Nursing: Mary Ann Rosa MSN, RN, CS, GNPDocument66 paginiIntroduction and Overview of Community Health Nursing: Mary Ann Rosa MSN, RN, CS, GNPphoenix18075% (4)
- Solomon Sallfors: Ambulatory Morning Report 1: AcneDocument3 paginiSolomon Sallfors: Ambulatory Morning Report 1: AcneSolomon Seth SallforsÎncă nu există evaluări
- SOAP NotesDocument4 paginiSOAP Notesemmag79Încă nu există evaluări
- Pharmacology of Drugs For AnemiaDocument49 paginiPharmacology of Drugs For AnemiaTeus Fatamorgana100% (2)
- 3 Treatment of HypertensionDocument7 pagini3 Treatment of HypertensiontiaraÎncă nu există evaluări
- Pulmonary Diseases - Dental ManagementDocument45 paginiPulmonary Diseases - Dental Managementfilyouth4life100% (3)
- Chapter 11. Colds and AllergyDocument22 paginiChapter 11. Colds and AllergyMonica CiorneiÎncă nu există evaluări
- Stroke - Final ReportDocument16 paginiStroke - Final ReportgolokipokÎncă nu există evaluări
- Rational Drug Prescribing Training CourseDocument78 paginiRational Drug Prescribing Training CourseAhmadu Shehu MohammedÎncă nu există evaluări
- IvabradineDocument33 paginiIvabradinepashaÎncă nu există evaluări
- Peptic Ulcer A Review On Etiology and PathogenesisDocument5 paginiPeptic Ulcer A Review On Etiology and PathogenesisEsti Suryani Haro MuntheÎncă nu există evaluări
- UTIDocument17 paginiUTIBongkotchakorn Mind PhonchaiÎncă nu există evaluări
- Frando Detailed Learning Module 3Document7 paginiFrando Detailed Learning Module 3Ranz Kenneth G. FrandoÎncă nu există evaluări
- Gastro MnemonicsDocument8 paginiGastro MnemonicsRufina SoomroÎncă nu există evaluări
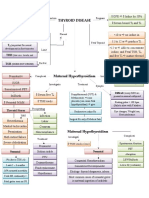
- Thyroid DiseaseDocument1 paginăThyroid DiseaseZiyadÎncă nu există evaluări
- Allergic Disorder: Dadan Surysaputra 20710031Document22 paginiAllergic Disorder: Dadan Surysaputra 20710031Dadan SuryasaputraÎncă nu există evaluări
- Soap Notes HypertensionDocument6 paginiSoap Notes HypertensionCHRISTINE KARENDIÎncă nu există evaluări
- Interview Pa Tool.Document5 paginiInterview Pa Tool.Raisah Bint AbdullahÎncă nu există evaluări
- Generic Name Brand Names Common Uses Possible Side Effects Mechanism of ActionDocument13 paginiGeneric Name Brand Names Common Uses Possible Side Effects Mechanism of Actionangel3424Încă nu există evaluări
- Sjogren'S Syndrome: Guided By: Dr. Richa MohanDocument17 paginiSjogren'S Syndrome: Guided By: Dr. Richa MohanAnkyÎncă nu există evaluări
- Descriptive Chart - Proteus VulgarisDocument2 paginiDescriptive Chart - Proteus Vulgariscrazybobblaskey0% (1)
- Pud Case StudyDocument8 paginiPud Case Studyapi-346620455Încă nu există evaluări
- GI Diarrheal Micro ChartDocument3 paginiGI Diarrheal Micro ChartEvan MillerÎncă nu există evaluări
- Approach To The Child With Anemia - UpToDateDocument41 paginiApproach To The Child With Anemia - UpToDateDaniel Enrique CardenasÎncă nu există evaluări
- PedquestDocument120 paginiPedquests1234321Încă nu există evaluări
- PATIENT 1 Nursing Assessment FormDocument5 paginiPATIENT 1 Nursing Assessment FormndemboloveÎncă nu există evaluări
- Patho Test 3Document7 paginiPatho Test 3Stephanie 'Sveen' HansenÎncă nu există evaluări
- Case Study #1 ScenarioDocument12 paginiCase Study #1 ScenarioHMG TVÎncă nu există evaluări
- A Step by Step Guide To Using Your Lantus Solostar PENDocument7 paginiA Step by Step Guide To Using Your Lantus Solostar PENGita Kusumadiani HaryonoÎncă nu există evaluări
- Lucentis Ad PDFDocument2 paginiLucentis Ad PDFvrtwpiÎncă nu există evaluări
- SSRIs and Athletic PerformanceDocument4 paginiSSRIs and Athletic PerformanceGuille monsterÎncă nu există evaluări
- Bookdrug Classification 3 KDocument150 paginiBookdrug Classification 3 KRobert Kikah0% (1)
- Using Virtual Screening Methods To Identify Small Molecule Inhibitors of PCSK9 and Prevent Heart DiseaseDocument40 paginiUsing Virtual Screening Methods To Identify Small Molecule Inhibitors of PCSK9 and Prevent Heart DiseaseRohan Arora3% (34)
- Himalaya HerbalsDocument45 paginiHimalaya HerbalsShraddha50% (2)
- Phosphate Vs Bicarbonate BuffersDocument11 paginiPhosphate Vs Bicarbonate BuffersSayuj NathÎncă nu există evaluări
- Drugs and Cosmetics Act, 1940 and Rules, 1945Document96 paginiDrugs and Cosmetics Act, 1940 and Rules, 1945Chandrashekhar Singh100% (3)
- Impact of Trips On Indian IndustryDocument33 paginiImpact of Trips On Indian IndustrymadhurendrahraÎncă nu există evaluări
- Validation of A Method For The Quantitation of Mdma in Seized Materials by Spectrophotometric MethodDocument6 paginiValidation of A Method For The Quantitation of Mdma in Seized Materials by Spectrophotometric MethodalbertuÎncă nu există evaluări
- IB Chemistry - Analysis of Aspirin Tablets PDFDocument2 paginiIB Chemistry - Analysis of Aspirin Tablets PDFScott GreenÎncă nu există evaluări
- Ibufen 600 Caplets: Summary of Product CharacteristicsDocument13 paginiIbufen 600 Caplets: Summary of Product Characteristicsddandan_2Încă nu există evaluări
- Molecular Networking As A Drug Discovery, Drug Metabolism, and Precision Medicine StrategyDocument12 paginiMolecular Networking As A Drug Discovery, Drug Metabolism, and Precision Medicine StrategySam SonÎncă nu există evaluări
- Pharmacology Tyroid and Antitiroid HormonDocument21 paginiPharmacology Tyroid and Antitiroid HormonPuterinugraha Wanca ApatyaÎncă nu există evaluări
- The NewsMaker - December, 2013Document44 paginiThe NewsMaker - December, 2013shankarswaminathanÎncă nu există evaluări
- Cluster Headache - ClinicalKeyDocument41 paginiCluster Headache - ClinicalKeyKhairunisaÎncă nu există evaluări
- MICHAELs P DRUG Nama ObatDocument7 paginiMICHAELs P DRUG Nama Obatbiondi siahaanÎncă nu există evaluări
- Journal Reading: Oleh: M. Isyhaduul Islam Arifiana Khusnul Hidayati Ulfi Shofahati Puskesmas GedongtengenDocument17 paginiJournal Reading: Oleh: M. Isyhaduul Islam Arifiana Khusnul Hidayati Ulfi Shofahati Puskesmas GedongtengenIka Wardhani KaruniaÎncă nu există evaluări
- MinoxidilDocument4 paginiMinoxidilapi-3797941100% (1)
- FDA - IDMP Webinar 2019Document73 paginiFDA - IDMP Webinar 2019Jose De La Cruz De La OÎncă nu există evaluări
- Rustom Shams PDFDocument48 paginiRustom Shams PDFmtaha85Încă nu există evaluări
- Presentation Musa NserekoDocument53 paginiPresentation Musa NserekogeekindiaÎncă nu există evaluări
- Chemistry JokesDocument3 paginiChemistry JokesDharline Abbygale Garvida AgullanaÎncă nu există evaluări
- CTD Open CefoperazoneDocument83 paginiCTD Open CefoperazoneSarfarazpk1Încă nu există evaluări
- BNF For Children (BNFC) 2018-2019 (Year 2018-2019) : Advance Book InformationDocument1 paginăBNF For Children (BNFC) 2018-2019 (Year 2018-2019) : Advance Book InformationKhaing Moh Moh ZinÎncă nu există evaluări
- The 10 Most Addictive Pain MedicationsDocument17 paginiThe 10 Most Addictive Pain MedicationslabendetÎncă nu există evaluări
- Tenpa L Et Al 2005 Gso Ba Rig Pa The Science of HealingDocument175 paginiTenpa L Et Al 2005 Gso Ba Rig Pa The Science of Healingབློ་བཟང་བརྟན་པ་Încă nu există evaluări
- IV Compatibility Chart (PDF Library)Document19 paginiIV Compatibility Chart (PDF Library)Lynda PerryÎncă nu există evaluări
- 079 BorseDocument9 pagini079 BorsepuriwatiÎncă nu există evaluări