S-ar putea să vă placă și
- Facial AnatomyDocument11 paginiFacial AnatomySneha SthaÎncă nu există evaluări
- Alternative Method For Fabrication of Power ArmDocument2 paginiAlternative Method For Fabrication of Power ArmVikas VatsÎncă nu există evaluări
- Evoked PotentialDocument6 paginiEvoked PotentialVikas VatsÎncă nu există evaluări
- Pikos-Mandibluar Block Autografts For Alveolar Ridge AugmentationDocument17 paginiPikos-Mandibluar Block Autografts For Alveolar Ridge AugmentationVikas VatsÎncă nu există evaluări
- BJOMS 2011. Technical Note. Use of Methylene Blue For Precise Peripheral Ostectomy of Keratocystic Odontogenic TumourDocument2 paginiBJOMS 2011. Technical Note. Use of Methylene Blue For Precise Peripheral Ostectomy of Keratocystic Odontogenic TumourVikas Vats100% (1)
- Vestibuloplasty With Skin Grafting and Lowering of The-HandoutDocument6 paginiVestibuloplasty With Skin Grafting and Lowering of The-HandoutVikas VatsÎncă nu există evaluări
- HN 03-2011 Submadibular Salivary Gland Transfer PDFDocument7 paginiHN 03-2011 Submadibular Salivary Gland Transfer PDFVikas VatsÎncă nu există evaluări
- 1545 1569 (2000) 037 0243:amouof 2.3.co 2Document5 pagini1545 1569 (2000) 037 0243:amouof 2.3.co 2Vikas VatsÎncă nu există evaluări
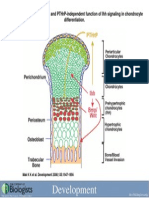
- Development 2008 Jun 135 (11) 1947-56, Fig. 7.Document1 paginăDevelopment 2008 Jun 135 (11) 1947-56, Fig. 7.Vikas VatsÎncă nu există evaluări
- Computer-Assisted Navigational Surgery in Oral and Maxillofacial SurgeryDocument9 paginiComputer-Assisted Navigational Surgery in Oral and Maxillofacial SurgeryVikas VatsÎncă nu există evaluări
- Acute Effects of Radiation InjuryDocument8 paginiAcute Effects of Radiation InjuryVikas VatsÎncă nu există evaluări
- Rhinoplasty Dissection ManualDocument185 paginiRhinoplasty Dissection ManualVikas Vats100% (3)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Module 4 (Basics of Sti, Hiv & Aids)Document37 paginiModule 4 (Basics of Sti, Hiv & Aids)Marky RoqueÎncă nu există evaluări
- Michelle L. Smith: Curriculum VitaeDocument5 paginiMichelle L. Smith: Curriculum Vitaeapi-327120894Încă nu există evaluări
- BasicsOfRadiopharmacy PDFDocument205 paginiBasicsOfRadiopharmacy PDFFithriana RachmawatiÎncă nu există evaluări
- Drug Card ZantacDocument1 paginăDrug Card ZantacAdrianne Bazo100% (1)
- Information To Be Included Within A Coal Mining Risk AssessmentDocument2 paginiInformation To Be Included Within A Coal Mining Risk AssessmentAlf HorsemanÎncă nu există evaluări
- Reteplase (MIRel)Document23 paginiReteplase (MIRel)Jhoann JamanilaÎncă nu există evaluări
- Behavior Therapy Research PaperDocument8 paginiBehavior Therapy Research PaperAmoni AzziÎncă nu există evaluări
- Preoperative Planning For Primary Total Hip ArthroplastyDocument8 paginiPreoperative Planning For Primary Total Hip Arthroplastyanon_683301094Încă nu există evaluări
- Oncology Nursing: Detection and Prevention of CancerDocument14 paginiOncology Nursing: Detection and Prevention of CancerEdwin Delos Reyes AbuÎncă nu există evaluări
- Behaviour Therapy: Amity Institute of Psychology and Allied SciencesDocument16 paginiBehaviour Therapy: Amity Institute of Psychology and Allied SciencesCharmoli Apum KhrimeÎncă nu există evaluări
- Exercise Therapy AssignmentDocument4 paginiExercise Therapy AssignmentApoorvÎncă nu există evaluări
- Decup 2014Document8 paginiDecup 2014Elija BrockÎncă nu există evaluări
- Jurnal SkoliosisDocument9 paginiJurnal SkoliosisLidya SiahaanÎncă nu există evaluări
- Disturbed Sleep PatternDocument2 paginiDisturbed Sleep PatternNiel Dela Cruz86% (7)
- Efektifitas Latihan Progressive Muscle Relaxation (PMR) Terhadap Mual Muntah Kemoterapi Pasien Kanker OvariumDocument8 paginiEfektifitas Latihan Progressive Muscle Relaxation (PMR) Terhadap Mual Muntah Kemoterapi Pasien Kanker OvariumMutmin AnsariÎncă nu există evaluări
- NCP PcapDocument1 paginăNCP PcapLhexie CooperÎncă nu există evaluări
- Life History of Dr.J.T. KentDocument13 paginiLife History of Dr.J.T. KentPrathibha MadikiÎncă nu există evaluări
- Comparison of Muscle Force Production Using Smith Machine and Free Weights (Bench Press and Squats) Cotterman 2005Document8 paginiComparison of Muscle Force Production Using Smith Machine and Free Weights (Bench Press and Squats) Cotterman 2005cleberÎncă nu există evaluări
- Rheynanda (2011316059) EssayDocument2 paginiRheynanda (2011316059) EssayRhey RYNÎncă nu există evaluări
- Angiofibroma Pic 2012 12 BDocument55 paginiAngiofibroma Pic 2012 12 Bkhairanifahma100% (1)
- What Is Alzheimer's - Alzheimer's AssociationDocument6 paginiWhat Is Alzheimer's - Alzheimer's AssociationRatnaPrasadNalamÎncă nu există evaluări
- Pharmacology and Therapeutics in Dentistry: Periodontology 2000Document2 paginiPharmacology and Therapeutics in Dentistry: Periodontology 2000BimalKrishnaÎncă nu există evaluări
- CARDOSO Et Al 2010 - Propolis Staphylo e Malassezia - Otite CaninaDocument3 paginiCARDOSO Et Al 2010 - Propolis Staphylo e Malassezia - Otite CaninaDébora SakiyamaÎncă nu există evaluări
- ASEA Athletics VT StudyDocument5 paginiASEA Athletics VT Studyalien asterixÎncă nu există evaluări
- Mood DisordersDocument1 paginăMood DisordersTeresa MartinsÎncă nu există evaluări
- Case Study of Neurological DisordersDocument10 paginiCase Study of Neurological DisordersSkyerexÎncă nu există evaluări
- Respiratory QuestionnaireDocument2 paginiRespiratory QuestionnaireMadhu SudhanÎncă nu există evaluări
- Rees Et Al-2019-Neurourology and UrodynamicsDocument9 paginiRees Et Al-2019-Neurourology and UrodynamicsMIHAELAÎncă nu există evaluări
- Dialysis Nurse Responsibilities and DutiesDocument22 paginiDialysis Nurse Responsibilities and DutiesWyn Agustin0% (1)
- Practice Guidelines For Telemental HealthDocument51 paginiPractice Guidelines For Telemental HealthNataanatiÎncă nu există evaluări