S-ar putea să vă placă și
- Guaifenesin and Dextromethorphan 01Document7 paginiGuaifenesin and Dextromethorphan 01not perfectÎncă nu există evaluări
- Asthma Action PlanDocument1 paginăAsthma Action PlanAkosÎncă nu există evaluări
- Asthma in ChildrenDocument3 paginiAsthma in Childrenwaikit0822Încă nu există evaluări
- Zafirlukast-for-asthma-prevention-2Document2 paginiZafirlukast-for-asthma-prevention-2William ImpÎncă nu există evaluări
- Under 5s Asthma Action PlanDocument5 paginiUnder 5s Asthma Action Planasimnaqvi2003Încă nu există evaluări
- DX StdieDocument22 paginiDX Stdietimie_reyesÎncă nu există evaluări
- PrednisoloneDocument4 paginiPrednisoloneUmemura-san SOkmo100% (1)
- GENERIC NAME: Terbutaline Drug Class and MechanismDocument4 paginiGENERIC NAME: Terbutaline Drug Class and MechanismAngel DamoÎncă nu există evaluări
- Pil 850Document9 paginiPil 850BarosPratamaÎncă nu există evaluări
- DYSNEA ASSESSMENTDocument2 paginiDYSNEA ASSESSMENTKang Opik TaufikÎncă nu există evaluări
- Aspirin and DipyridamoleDocument6 paginiAspirin and DipyridamoleRoxana Aldea-CiaciruÎncă nu există evaluări
- OndansetronDocument11 paginiOndansetronIlyes FerenczÎncă nu există evaluări
- Integrated Prevention and Management of Selected Acute and Chronic Illness (IPMSACI) - Job AidDocument9 paginiIntegrated Prevention and Management of Selected Acute and Chronic Illness (IPMSACI) - Job AidCOMDIS-HSDÎncă nu există evaluări
- BRAND NAME (S) : Unasyn: Generic Name: Ampicillin/Sulbactam - Injection (Am-Pi-Sil-In/Sul-BAK-tam)Document2 paginiBRAND NAME (S) : Unasyn: Generic Name: Ampicillin/Sulbactam - Injection (Am-Pi-Sil-In/Sul-BAK-tam)Oliver BagarinaoÎncă nu există evaluări
- Drug Details PDFDocument4 paginiDrug Details PDFElÎncă nu există evaluări
- Augmentin: Generic Name (S) : Amoxicillin/Potassium ClavulanateDocument5 paginiAugmentin: Generic Name (S) : Amoxicillin/Potassium ClavulanateramkumarÎncă nu există evaluări
- Propranolol For HemangiomaDocument4 paginiPropranolol For HemangiomaJheelzy DatorÎncă nu există evaluări
- Respiratory Responding To Symptoms OtcDocument2 paginiRespiratory Responding To Symptoms Otcciaraburns003Încă nu există evaluări
- Asthma - Discharge Care For Adults - EnglishDocument2 paginiAsthma - Discharge Care For Adults - EnglishMalik Khuram ShazadÎncă nu există evaluări
- Prescription Label: AtenololDocument3 paginiPrescription Label: AtenololRafiÎncă nu există evaluări
- Chlorpheniramine - MedlinePlus Drug InformationDocument11 paginiChlorpheniramine - MedlinePlus Drug InformationKhawar NagraÎncă nu există evaluări
- Cephradine, MefenamicDocument4 paginiCephradine, MefenamicSarah GatuzÎncă nu există evaluări
- Sere TideDocument6 paginiSere TideCarinaPuspitaKadarwennyÎncă nu există evaluări
- Patient - Information - Leaflet 3698 Flixotide Evohaler 50 Uk - PDF 1510756509Document8 paginiPatient - Information - Leaflet 3698 Flixotide Evohaler 50 Uk - PDF 1510756509Nicoleta BratosinÎncă nu există evaluări
- Lecture 2 NDHDocument4 paginiLecture 2 NDHTricia Jane OpinaldoÎncă nu există evaluări
- Cefuroxime (Oral Route) : US Brand NamesDocument9 paginiCefuroxime (Oral Route) : US Brand NamesYaleswari Hayu PertiwiÎncă nu există evaluări
- SOP VerifikasoDocument85 paginiSOP Verifikasofransiska labuÎncă nu există evaluări
- R-Cin Suspension LeafletDocument8 paginiR-Cin Suspension LeafletPuneet KhannaÎncă nu există evaluări
- Adult Asthma Self-Management Plan (98825) - tcm88-727793Document2 paginiAdult Asthma Self-Management Plan (98825) - tcm88-727793Mimi afiqah KasimÎncă nu există evaluări
- Theophylline Medication Guide for COPD TreatmentDocument3 paginiTheophylline Medication Guide for COPD TreatmentvidiaprajnaÎncă nu există evaluări
- Prescription Label: TrazodoneDocument3 paginiPrescription Label: TrazodoneImperial Beach Pet Hospital IBPHÎncă nu există evaluări
- Case Study 1Document3 paginiCase Study 1Amberly BohackÎncă nu există evaluări
- Housejob GuideDocument11 paginiHousejob GuideSam James100% (1)
- IMCI Job-Aid Users' Manual: Integrated Management of Childhood Illness (Imci) : Age 0 To 2 MonthsDocument1 paginăIMCI Job-Aid Users' Manual: Integrated Management of Childhood Illness (Imci) : Age 0 To 2 MonthsCOMDIS-HSDÎncă nu există evaluări
- Paed Anaesthetic 01Document3 paginiPaed Anaesthetic 01Mafeitzeral MamatÎncă nu există evaluări
- HP8865 Using Paracetamol or IbuprofenDocument7 paginiHP8865 Using Paracetamol or IbuprofenRoti Toti100% (1)
- Pil 1503Document6 paginiPil 1503Zohair ShaheerÎncă nu există evaluări
- Medication Information For Parents and Teachers: Amphetamine-Dexedrine, Procentra, Zenzedi, Adderall, VyvanseDocument10 paginiMedication Information For Parents and Teachers: Amphetamine-Dexedrine, Procentra, Zenzedi, Adderall, VyvanseMonique WrightÎncă nu există evaluări
- Physical and LanguageDocument5 paginiPhysical and LanguagecatalinatdelarosaÎncă nu există evaluări
- Dulcan Effexor PristiqDocument8 paginiDulcan Effexor PristiqMonique WrightÎncă nu există evaluări
- Cyanocobalamin Memorial Sloan Kettering Cancer Center - CyanocobalaminDocument9 paginiCyanocobalamin Memorial Sloan Kettering Cancer Center - CyanocobalaminpatgarettÎncă nu există evaluări
- Ibuprofen Headache Menstrual Cramps Arthritis: How To Use Ibuprofen OralDocument6 paginiIbuprofen Headache Menstrual Cramps Arthritis: How To Use Ibuprofen OralsakuraleeshaoranÎncă nu există evaluări
- Virina, Wella S. BSN Ii Pharmacology Critical ThinkingDocument5 paginiVirina, Wella S. BSN Ii Pharmacology Critical ThinkingEllee HadesÎncă nu există evaluări
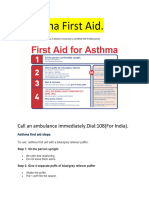
- Asthama First Aid.Document3 paginiAsthama First Aid.Manoj KumarÎncă nu există evaluări
- Ot RivinDocument6 paginiOt Rivinธัญญภัทร์ ทะหมุนÎncă nu există evaluări
- Medicine CompleteDocument93 paginiMedicine CompletefdjslajfÎncă nu există evaluări
- Paper 2 ChlorphenamineDocument4 paginiPaper 2 Chlorphenaminenurfitriani annisaÎncă nu există evaluări
- Anti Spasmodic MedicationsDocument2 paginiAnti Spasmodic MedicationsPhan Do Dang KhoaÎncă nu există evaluări
- Phenyl Eph Rine 1Document6 paginiPhenyl Eph Rine 1rayalarasatitiÎncă nu există evaluări
- COPD Flare-Up Action Plan: Green Zone: My COPD Is Well ControlledDocument2 paginiCOPD Flare-Up Action Plan: Green Zone: My COPD Is Well ControlledAlex MonaghanÎncă nu există evaluări
- Patient Information Series: Pulmonary Function Testing in ChildrenDocument2 paginiPatient Information Series: Pulmonary Function Testing in Childrendicky wahyudiÎncă nu există evaluări
- Albiglutide Patient HandoutDocument4 paginiAlbiglutide Patient HandoutHannaÎncă nu există evaluări
- Pediatricreferencecard 04Document2 paginiPediatricreferencecard 04yesumovsÎncă nu există evaluări
- Year 9 Camp Health and Medical ConsentDocument3 paginiYear 9 Camp Health and Medical ConsentFiona CharringtonÎncă nu există evaluări
- Salmeterol-inhaler-for-asthma-1Document3 paginiSalmeterol-inhaler-for-asthma-1William ImpÎncă nu există evaluări
- Explanation StationDocument4 paginiExplanation StationjsdlzjÎncă nu există evaluări
- Ace Tamino FenDocument2 paginiAce Tamino FenfranklinÎncă nu există evaluări
- Drug Study CardinalDocument21 paginiDrug Study CardinalDrei LanuzoÎncă nu există evaluări
- d12 AustraliaNZDocument10 paginid12 AustraliaNZPaeyuu AuÎncă nu există evaluări
- PRIMARY CARE PRACTICE EXAMSDocument23 paginiPRIMARY CARE PRACTICE EXAMSDanny Irung100% (3)
- PRIMARY CARE PRACTICE EXAMSDocument23 paginiPRIMARY CARE PRACTICE EXAMSDanny Irung100% (3)
- d12 AustraliaNZDocument10 paginid12 AustraliaNZPaeyuu AuÎncă nu există evaluări
- Speaking Skills Tofel TestDocument11 paginiSpeaking Skills Tofel TestPaeyuu AuÎncă nu există evaluări
- BudesonideDocument4 paginiBudesonideapi-3797941Încă nu există evaluări
- Daftar Permintaan Pustu-2Document15 paginiDaftar Permintaan Pustu-2Yanti FitryÎncă nu există evaluări
- Form Stok OpnameDocument14 paginiForm Stok OpnameYena TaherÎncă nu există evaluări
- Treating Thyroid Disorders in Elderly PatientsDocument9 paginiTreating Thyroid Disorders in Elderly PatientsKen RegalaÎncă nu există evaluări
- 50 Item Pharmacology ExamDocument10 pagini50 Item Pharmacology Examshark_tale04100% (1)
- KramerDocument4 paginiKramerChandanMatoliaÎncă nu există evaluări
- Drug Card Emergency DepartmentDocument2 paginiDrug Card Emergency Departmentdrmohdtanveer100% (3)
- Comparison of Dexmedetomidine, Pethidine and Tramadol in The Treatment of Post-Neuraxial Anaesthesia ShiveringDocument6 paginiComparison of Dexmedetomidine, Pethidine and Tramadol in The Treatment of Post-Neuraxial Anaesthesia ShiveringabdulÎncă nu există evaluări
- A Simple RP-HPLC Method For Simultaneous Analysis of Paracetmol, Nimesulide and Tizanidine Hydrochloride in Pharmaceutical Dosage FormsDocument9 paginiA Simple RP-HPLC Method For Simultaneous Analysis of Paracetmol, Nimesulide and Tizanidine Hydrochloride in Pharmaceutical Dosage FormsHanimi ReddyÎncă nu există evaluări
- CARDIOVASCULAR AND DIGESTIVE MEDICINESDocument15 paginiCARDIOVASCULAR AND DIGESTIVE MEDICINESDovan Anfield GenkÎncă nu există evaluări
- PDFDocument732 paginiPDFMahmud Eljaarani89% (9)
- Vademecum Valesalud 201401Document42 paginiVademecum Valesalud 201401petacosÎncă nu există evaluări
- Sida Cordifolia (Linn) - An OverviewDocument8 paginiSida Cordifolia (Linn) - An Overviewjiva_shakti0Încă nu există evaluări
- Greer Citizen E-Edition 12.14.16Document16 paginiGreer Citizen E-Edition 12.14.16greercitizenÎncă nu există evaluări
- Concept Map Template NURS 3073Document3 paginiConcept Map Template NURS 3073Savanna ChambersÎncă nu există evaluări
- Andrews' Chapter 13 David M. Bracciano, D.ODocument93 paginiAndrews' Chapter 13 David M. Bracciano, D.OErianaSari100% (2)
- AntacidDocument5 paginiAntacidRohan TutlaniÎncă nu există evaluări
- Medication Errors: What They Are, How They Happen, and How To Avoid ThemDocument9 paginiMedication Errors: What They Are, How They Happen, and How To Avoid ThemMoisesÎncă nu există evaluări
- MCQquestionsDocument2 paginiMCQquestionsapi-26291651100% (6)
- Drug Interactions Literature ReviewDocument2 paginiDrug Interactions Literature ReviewFitri AnggraeniÎncă nu există evaluări
- Indian DrummersDocument4 paginiIndian DrummersAbdul MarufÎncă nu există evaluări
- Antidepressant ChartDocument7 paginiAntidepressant Chartinher1tance100% (4)
- Pp2 AnswersDocument4 paginiPp2 AnswersDallis HodgsonÎncă nu există evaluări
- Opioid Induced HyperalgesiaDocument39 paginiOpioid Induced HyperalgesiaAnonymous XEbh4UxfÎncă nu există evaluări
- Hospital Admission and Discharge ProceduresDocument4 paginiHospital Admission and Discharge Proceduresmftaganas100% (2)
- Ceftriaxone Ringer LactatDocument11 paginiCeftriaxone Ringer Lactatmahatir muhammadÎncă nu există evaluări
- Ra 10918Document19 paginiRa 10918ryuureccaÎncă nu există evaluări
- About This List DosingDocument15 paginiAbout This List DosingAla AbushehabÎncă nu există evaluări
- Tramadol: (Trade Names: Ultram®, Ultracet®)Document1 paginăTramadol: (Trade Names: Ultram®, Ultracet®)Marthaluzy CarinaÎncă nu există evaluări