S-ar putea să vă placă și
- Qpowieueuyrtbzmlakjjhfgftryeiwpqpqpqpqpqpqpqpqppppppppppppppppppppppp PPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPQQQQQQQQQQQQQQQQ QQQQQQQQQQQQQQQQQQQQPQPQPQPQPDocument1 paginăQpowieueuyrtbzmlakjjhfgftryeiwpqpqpqpqpqpqpqpqppppppppppppppppppppppp PPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPQQQQQQQQQQQQQQQQ QQQQQQQQQQQQQQQQQQQQPQPQPQPQPzano_adamÎncă nu există evaluări
- Is Evolutionary Theory Central To Molecular Cell Biology?: Neil W. BlackstoneDocument10 paginiIs Evolutionary Theory Central To Molecular Cell Biology?: Neil W. BlackstoneDita Ayu FaradilaÎncă nu există evaluări
- JCMB V7N1 V8N2Document96 paginiJCMB V7N1 V8N2zano_adamÎncă nu există evaluări
- Management of Chronic Suppurative Otitis Media (CSOM) in High-Risk PopulationsDocument1 paginăManagement of Chronic Suppurative Otitis Media (CSOM) in High-Risk PopulationsBhara Julyandhika IrdiÎncă nu există evaluări
- SMDocument1 paginăSMzano_adamÎncă nu există evaluări
- Treating Chronic Paroxysmal HemicraniaDocument23 paginiTreating Chronic Paroxysmal HemicraniaAmelia GunawanÎncă nu există evaluări
- AHS AAN GuidelinesDocument16 paginiAHS AAN GuidelinesAlejandra CastilloÎncă nu există evaluări
- 1200 Walker MelissaDocument55 pagini1200 Walker Melissazano_adamÎncă nu există evaluări
- Congnital Hipotiroid Journal of Rare Disease PDFDocument22 paginiCongnital Hipotiroid Journal of Rare Disease PDFJenny SchneiderÎncă nu există evaluări
- 1 PDFDocument12 pagini1 PDFzano_adamÎncă nu există evaluări
- 1Document6 pagini1zano_adamÎncă nu există evaluări
- DAFTAR PUSTAKA Nasofaring Tumor ReferencesDocument1 paginăDAFTAR PUSTAKA Nasofaring Tumor Referenceszano_adamÎncă nu există evaluări
- Carcinoma Nasopharynx ChintiaDocument10 paginiCarcinoma Nasopharynx ChintiaChintia R. EndismoyoÎncă nu există evaluări
- Tetanus BagusDocument11 paginiTetanus BagusArief Yudho PrabowoÎncă nu există evaluări
- 2314 FullDocument15 pagini2314 Fullzano_adamÎncă nu există evaluări
- AddDocument1 paginăAddzano_adamÎncă nu există evaluări
- Amj 06 371Document3 paginiAmj 06 371zano_adamÎncă nu există evaluări
- Clinical Practice GuidelinesDocument3 paginiClinical Practice Guidelineszano_adamÎncă nu există evaluări
- Management of Chronic Suppurative Otitis Media (CSOM) in High-Risk PopulationsDocument1 paginăManagement of Chronic Suppurative Otitis Media (CSOM) in High-Risk PopulationsBhara Julyandhika IrdiÎncă nu există evaluări
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 2000)Document7 paginiP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 2000)zano_adamÎncă nu există evaluări
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 2000)Document7 paginiP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 2000)zano_adamÎncă nu există evaluări
- Epidemio Etio CA NasofaringDocument9 paginiEpidemio Etio CA Nasofaringzano_adamÎncă nu există evaluări
- Carcinoma Nasopharynx ChintiaDocument10 paginiCarcinoma Nasopharynx ChintiaChintia R. EndismoyoÎncă nu există evaluări
- Otitis MediaDocument84 paginiOtitis MediaAlex MatthewÎncă nu există evaluări
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 2000)Document9 paginiP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 2000)zano_adamÎncă nu există evaluări
- Semiotics Is The Study of SignsDocument7 paginiSemiotics Is The Study of Signszano_adamÎncă nu există evaluări
- Peritonsillar AbscessDocument4 paginiPeritonsillar Abscessbe_jhoniÎncă nu există evaluări
- JKL 2Document8 paginiJKL 2zano_adamÎncă nu există evaluări
- AaaaDocument1 paginăAaaazano_adamÎncă nu există evaluări
- JKL4Document17 paginiJKL4zano_adamÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Focused Muscular Tension PDFDocument16 paginiFocused Muscular Tension PDFMori Trump100% (1)
- Cebu Bio Medical Medical SuppliesDocument78 paginiCebu Bio Medical Medical SuppliesguaporicÎncă nu există evaluări
- AD&D 1.0 I5 Level 7-9 Adventure - Lost Tomb of MartekDocument86 paginiAD&D 1.0 I5 Level 7-9 Adventure - Lost Tomb of MartekSamuel Gomes90% (10)
- EYP Teambuilding Guide - FinlandDocument21 paginiEYP Teambuilding Guide - FinlandMircea PetrescuÎncă nu există evaluări
- Crochet Now March 2019Document128 paginiCrochet Now March 2019Chris Chrys100% (23)
- Keiraku To Keiketsu Meridians and Acupoints As Described in Japanese Kanp Medicine PDFDocument45 paginiKeiraku To Keiketsu Meridians and Acupoints As Described in Japanese Kanp Medicine PDFenfermeironilson6321Încă nu există evaluări
- 2019-06-01 Trapper and Predator CallerDocument58 pagini2019-06-01 Trapper and Predator Callerrobert allenÎncă nu există evaluări
- Developing Reading Power Grade IVDocument40 paginiDeveloping Reading Power Grade IVlulu91% (11)
- Act 1.2 Evolution of ManDocument3 paginiAct 1.2 Evolution of ManRay FaustinoÎncă nu există evaluări
- AT&T Alascom NetworkDocument1 paginăAT&T Alascom NetworkrbskoveÎncă nu există evaluări
- The Physics of Feldenkrais: Part 2: No Strain, No GainDocument9 paginiThe Physics of Feldenkrais: Part 2: No Strain, No GainvkÎncă nu există evaluări
- BattleMech Unit, Manufacturer, and Factory ListingDocument12 paginiBattleMech Unit, Manufacturer, and Factory ListingMarcel BuckebredeÎncă nu există evaluări
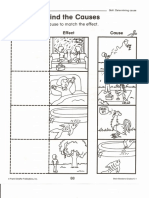
- 06 Cause and Effect PDFDocument17 pagini06 Cause and Effect PDFnewdragonvip06Încă nu există evaluări
- Bug GuideDocument25 paginiBug GuideHasbi AshshidiqqiÎncă nu există evaluări
- Abhuman Character Guide (07-15-15) PDFDocument62 paginiAbhuman Character Guide (07-15-15) PDFsigurdhart100% (2)
- Characterization and Evaluation of The Stunning Systems Used For Horses in ChileDocument9 paginiCharacterization and Evaluation of The Stunning Systems Used For Horses in ChileAnita CJÎncă nu există evaluări
- Anatomy Notes Upsc PDFDocument169 paginiAnatomy Notes Upsc PDFDEEJK100% (1)
- Kidc2b4s Box 4 Cambridge PDFDocument22 paginiKidc2b4s Box 4 Cambridge PDFElisabet Reinaga100% (1)
- Fish Mucus ResearchDocument5 paginiFish Mucus ResearchStephen SabinayÎncă nu există evaluări
- Understanding The Pit BullDocument2 paginiUnderstanding The Pit BullYazbeth Chan GarciaÎncă nu există evaluări
- Shodasha Ganapathi ListDocument2 paginiShodasha Ganapathi ListshripriyaaÎncă nu există evaluări
- Human anatomy & physiology sampler questionsDocument13 paginiHuman anatomy & physiology sampler questionsLauraLaine100% (3)
- Ancient SkinDocument2 paginiAncient Skinjoel lealÎncă nu există evaluări
- Understanding Culture, Society and Politics: First Quarter Module 4 - Week 4Document12 paginiUnderstanding Culture, Society and Politics: First Quarter Module 4 - Week 4Rose DiÎncă nu există evaluări
- Embriologia Del CerdoDocument11 paginiEmbriologia Del CerdoTadase Hotori0% (1)
- Manual Formular CnemeDocument620 paginiManual Formular CnemeDaniela TriteanuÎncă nu există evaluări
- Frog Muscle ProtocolDocument13 paginiFrog Muscle Protocolrjbagh08Încă nu există evaluări
- Shang Han LunDocument3 paginiShang Han Lunwuweitao50% (2)
- P Brevispinus 2015 FinalDocument6 paginiP Brevispinus 2015 FinalMark DinoÎncă nu există evaluări
- Fuss-Free Meals 35 Simple Skillet Recipes and One-Pot RecipesDocument40 paginiFuss-Free Meals 35 Simple Skillet Recipes and One-Pot Recipesajyh28100% (1)