S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Valvular Heart DiseaseDocument2 paginiValvular Heart DiseaseAnonymous TVk12eX4Încă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Heart Failure: Dr.K.Sathish Kumar, MD (Hom) .Document11 paginiHeart Failure: Dr.K.Sathish Kumar, MD (Hom) .mnr hmcÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- How To Write A Proposal EssayDocument3 paginiHow To Write A Proposal Essaypilav0wutyk3100% (2)
- The Heart LA WorksheetDocument4 paginiThe Heart LA Worksheeteas grade04Încă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Deviriligo Notes 12Document99 paginiDeviriligo Notes 12A Fish100% (1)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- 2008 Tale of The Seven MaresDocument9 pagini2008 Tale of The Seven MaresEduardo Alfredo Gutierrez PardoÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Precourse Self-Assessment ResultsDocument3 paginiPrecourse Self-Assessment ResultsDioseptyaÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Myocardial InfarctionDocument20 paginiMyocardial Infarctionshmily_0810100% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Hypertension LecturesDocument65 paginiHypertension LecturesAdebisiÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- BME 6480: Biomedical Instrumentation Jason Kabzinski, Alex Lau, Mounica Naraharisetti, Jody PaulanDocument22 paginiBME 6480: Biomedical Instrumentation Jason Kabzinski, Alex Lau, Mounica Naraharisetti, Jody PaulanMona NaiduÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Rhythm Control Versus Rate Control For Atrial FibrillationDocument5 paginiRhythm Control Versus Rate Control For Atrial FibrillationlowellaÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Tutorial 1Document8 paginiTutorial 1ALISYA SOPHIA MOHAMMAD ABU SHAHID CHRISÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Indications: PurposeDocument13 paginiIndications: PurposeIRA ODETTE GATUSÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- How To Do CPR On An AdultDocument25 paginiHow To Do CPR On An AdultabÎncă nu există evaluări
- BLS Study Guide and PretestDocument47 paginiBLS Study Guide and PretestRicha AbcedeÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Aha 2018 Cir.0000000000000558 PDFDocument426 paginiAha 2018 Cir.0000000000000558 PDFDesy YardinaÎncă nu există evaluări
- Pengambilan Darah Pada Pasien Dengan Akses Vena SulitDocument21 paginiPengambilan Darah Pada Pasien Dengan Akses Vena SulitHanny Siti NuraeniÎncă nu există evaluări
- Bls Study GuideDocument2 paginiBls Study GuideJohnÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Central Venous Pressure and Pulmonary Capillary Wedge Pressure MonitoringDocument6 paginiCentral Venous Pressure and Pulmonary Capillary Wedge Pressure MonitoringSuresh KumarÎncă nu există evaluări
- Medicine AnswersDocument6 paginiMedicine AnswersHarsha Vipin100% (5)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Hypertensive RetinopathyDocument30 paginiHypertensive Retinopathyhidayah BorhanudinÎncă nu există evaluări
- Pacemakers - Fact SheetDocument7 paginiPacemakers - Fact Sheettalha.k.rajpootÎncă nu există evaluări
- Cardio Vascular Assessment: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingDocument46 paginiCardio Vascular Assessment: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingmeghanaÎncă nu există evaluări
- CCrISP 7 Shock and HaemorrhageDocument27 paginiCCrISP 7 Shock and HaemorrhageDrSayk YousufÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Basic Life Support For Healthcare Providers (BLS) : Presented By: Youssef Youssef RT Respiratory Therapy DepartementDocument43 paginiBasic Life Support For Healthcare Providers (BLS) : Presented By: Youssef Youssef RT Respiratory Therapy Departementkurt94764Încă nu există evaluări
- Point of Care Ultrasound With Pocket Size Devices in Emergency Department - 2019Document10 paginiPoint of Care Ultrasound With Pocket Size Devices in Emergency Department - 2019ntnquynhproÎncă nu există evaluări
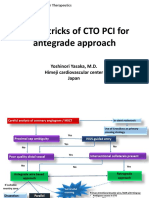
- Tips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanDocument21 paginiTips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanEll KlazureÎncă nu există evaluări
- THE CARDIOVASCULAR SYSTEM ReviewDocument34 paginiTHE CARDIOVASCULAR SYSTEM ReviewEndahÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Monology of StensenDocument1 paginăMonology of StensenmoonlightsoantaÎncă nu există evaluări
- Crao CrvoDocument2 paginiCrao Crvonizzah afinaÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)