S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Self-Assessment Quiz: Introduction To Epidemiology Page 1-85Document75 paginiSelf-Assessment Quiz: Introduction To Epidemiology Page 1-85Coy Nuñez100% (4)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- NCRA AJCC Cancer Staging Manual 8th Edition UpdateDocument61 paginiNCRA AJCC Cancer Staging Manual 8th Edition UpdateNancyLiao50% (2)
- The Pineal GlandDocument3 paginiThe Pineal GlandCharity Masters100% (2)
- Fatigue NCPDocument2 paginiFatigue NCPclydell joyce masiar100% (6)
- AnaemiaDocument83 paginiAnaemiaMohammad_Islam87100% (2)
- Morphopathology SET 16 Pathologies of The Gastrointestinal TractDocument29 paginiMorphopathology SET 16 Pathologies of The Gastrointestinal TractMohammad_Islam87Încă nu există evaluări
- Lecture 20 CarcinogenesisDocument84 paginiLecture 20 CarcinogenesisMohammad_Islam87100% (1)
- Morphopathology SET14 Respiratory Pathologies: by Qamar AhmadDocument18 paginiMorphopathology SET14 Respiratory Pathologies: by Qamar AhmadMohammad_Islam87Încă nu există evaluări
- Liver Curs 2009Document215 paginiLiver Curs 2009Mohammad_Islam87Încă nu există evaluări
- Morphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadDocument19 paginiMorphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadMohammad_Islam87Încă nu există evaluări
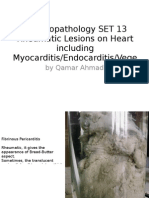
- Morphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeDocument25 paginiMorphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeMohammad_Islam87Încă nu există evaluări
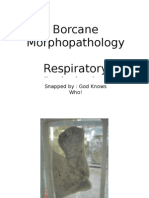
- Borcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarDocument11 paginiBorcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Încă nu există evaluări
- Borcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarDocument7 paginiBorcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Încă nu există evaluări
- Morphopathology SET 15 Renal Pathologies: by Qamar AhmadDocument25 paginiMorphopathology SET 15 Renal Pathologies: by Qamar AhmadMohammad_Islam87Încă nu există evaluări
- Morphopathology Macroscopy (Romanian-Batch)Document187 paginiMorphopathology Macroscopy (Romanian-Batch)Mohammad_Islam87100% (1)
- Borcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarDocument7 paginiBorcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87100% (1)
- Workshop 18Document4 paginiWorkshop 18Mohammad_Islam87Încă nu există evaluări
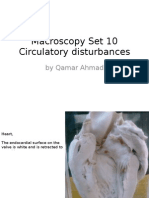
- Macroscopy Set 10 Circulatory Disturbances: by Qamar AhmadDocument55 paginiMacroscopy Set 10 Circulatory Disturbances: by Qamar AhmadMohammad_Islam87Încă nu există evaluări
- Workshop 20Document2 paginiWorkshop 20Mohammad_Islam87Încă nu există evaluări
- ?#ry%oefr: - J4 @,8/ MryDocument15 pagini?#ry%oefr: - J4 @,8/ MryMohammad_Islam87Încă nu există evaluări
- Workshop 19Document3 paginiWorkshop 19Mohammad_Islam87Încă nu există evaluări
- Physical Signs of The AbdomenDocument93 paginiPhysical Signs of The AbdomenaimanÎncă nu există evaluări
- Conditions Presenting With Abdominal PainDocument69 paginiConditions Presenting With Abdominal PainaimanÎncă nu există evaluări
- Morphopatholgy Set 9 Circulatory Disturbances: by Qamar AhmadDocument24 paginiMorphopatholgy Set 9 Circulatory Disturbances: by Qamar AhmadMohammad_Islam87Încă nu există evaluări
- Morphopathology Set 8 Melanocytic Tumors: by Qamar AhmadDocument54 paginiMorphopathology Set 8 Melanocytic Tumors: by Qamar AhmadMohammad_Islam87Încă nu există evaluări
- Morphopathology Set 11 Atherosclerosis and Other Cardiaovascular DisordersDocument21 paginiMorphopathology Set 11 Atherosclerosis and Other Cardiaovascular DisordersMohammad_Islam87Încă nu există evaluări
- Workshop 17Document4 paginiWorkshop 17Mohammad_Islam87Încă nu există evaluări
- Peptic Ulcer DiseaseDocument54 paginiPeptic Ulcer DiseaseMohammad_Islam87Încă nu există evaluări
- STOMACCURS2Document12 paginiSTOMACCURS2Mohammad_Islam87Încă nu există evaluări
- Stomach - GastritisDocument22 paginiStomach - GastritisaimanÎncă nu există evaluări
- Examination of AbdomenDocument41 paginiExamination of AbdomenMohammad_Islam87Încă nu există evaluări
- 01 Serpentina Presentation PDFDocument27 pagini01 Serpentina Presentation PDFabcÎncă nu există evaluări
- DelphiDocument28 paginiDelphiMEANMYFATHERAREONE100% (1)
- Human Reproduction: Type A: Multiple Choice QuestionsDocument7 paginiHuman Reproduction: Type A: Multiple Choice Questionsriya sharmaÎncă nu există evaluări
- Gadtc PHCDocument246 paginiGadtc PHCshawnÎncă nu există evaluări
- SEX CHANGE - Physically Impossible, Psychosocially Unhelpful, and Philosophically MisguidedDocument63 paginiSEX CHANGE - Physically Impossible, Psychosocially Unhelpful, and Philosophically MisguidedAntonio Bernard33% (3)
- NCP Drug CardDocument6 paginiNCP Drug CardlaniÎncă nu există evaluări
- Ignatavicius TOCDocument9 paginiIgnatavicius TOCjennaaahhhÎncă nu există evaluări
- Sports Massage Therapist - Sports Injury ChiropractorDocument3 paginiSports Massage Therapist - Sports Injury ChiropractorDr. Dale MacdonaldÎncă nu există evaluări
- Test Bank For Introduction To Medical Surgical Nursing 4th Edition Adrianne D Linton Full DownloadDocument12 paginiTest Bank For Introduction To Medical Surgical Nursing 4th Edition Adrianne D Linton Full Downloadmelissapollardoxieprwsdb100% (40)
- Intussusception Pedia ReportDocument13 paginiIntussusception Pedia ReportJesselyn HeruelaÎncă nu există evaluări
- Master Oral MedicineDocument54 paginiMaster Oral MedicineDr. MujahidÎncă nu există evaluări
- Genetics of Breast Cancer PDFDocument3 paginiGenetics of Breast Cancer PDFmohamedhazemelfollÎncă nu există evaluări
- Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDocument4 paginiPractice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses Central100% (1)
- Jamaica Times November 2014 WebDocument18 paginiJamaica Times November 2014 WebJamaica Times NewspaperÎncă nu există evaluări
- Science 10 Lesson PlanDocument7 paginiScience 10 Lesson PlanThesairah Taule100% (1)
- Advanced Special Subject 9.2Document22 paginiAdvanced Special Subject 9.2Nguyen Ngoc Khoi NguyenÎncă nu există evaluări
- Google LDN (E-Book)Document146 paginiGoogle LDN (E-Book)bktangoÎncă nu există evaluări
- Digestive Health & You - 03062018Document8 paginiDigestive Health & You - 03062018Times MediaÎncă nu există evaluări
- Masters Training in Reproductive Medicine and IVFDocument1 paginăMasters Training in Reproductive Medicine and IVFIBC Medical ServicesÎncă nu există evaluări
- Acute Ulcerative Stomatitis.Document5 paginiAcute Ulcerative Stomatitis.Manar AlsoltanÎncă nu există evaluări
- Patient Evaluation During The Anaesthesia in AnimalDocument3 paginiPatient Evaluation During The Anaesthesia in AnimalNabin NeupaneÎncă nu există evaluări
- Spleen and Liver Sur LecDocument14 paginiSpleen and Liver Sur LecYA M AYÎncă nu există evaluări
- Thyroid DiseaseDocument41 paginiThyroid DiseaseUday Kumar KolluriÎncă nu există evaluări
- Thyroid Gland NotesDocument21 paginiThyroid Gland NotesbryanÎncă nu există evaluări
- 1 Terminology II LectureDocument45 pagini1 Terminology II Lecturemaramaliii37Încă nu există evaluări
- Phytochemistry, Antioxidant and Antibacterial Activities of Medicinal Plants - A Comparative StudyDocument12 paginiPhytochemistry, Antioxidant and Antibacterial Activities of Medicinal Plants - A Comparative StudyRigotti BrÎncă nu există evaluări