S-ar putea să vă placă și
- Common Surgical PresentationsDocument49 paginiCommon Surgical PresentationsJeremiah HiiÎncă nu există evaluări
- Anti Infective Drug ChartDocument1 paginăAnti Infective Drug ChartJessica100% (1)
- Lydia Hall: Reporters: Gwenn Marielle Galdo Kristine CustodioDocument15 paginiLydia Hall: Reporters: Gwenn Marielle Galdo Kristine CustodioKristine CustodioÎncă nu există evaluări
- Is BN 9514269640Document99 paginiIs BN 9514269640balab2311Încă nu există evaluări
- Eva Madison Complex ReflectionDocument2 paginiEva Madison Complex ReflectionKyuSheen100% (1)
- Principles of Concrete Mix DesignDocument67 paginiPrinciples of Concrete Mix DesignAbu Mariam80% (5)
- Labor and Delivery MedsDocument12 paginiLabor and Delivery MedsSam DanaÎncă nu există evaluări
- AMC Online - Recalls - V3Document167 paginiAMC Online - Recalls - V3Halfida100% (3)
- GI Bleeding HXDocument3 paginiGI Bleeding HXBitu JaaÎncă nu există evaluări
- Remember: Goals and Plan of Care Should Be Base According To Client's Problems/needs NOT According To Your OwnDocument11 paginiRemember: Goals and Plan of Care Should Be Base According To Client's Problems/needs NOT According To Your Ownavinash dhameriyaÎncă nu există evaluări
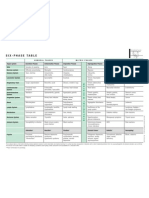
- Six-Phase Table: International Society of HomotoxicologyDocument1 paginăSix-Phase Table: International Society of HomotoxicologyPablo Matas SoriaÎncă nu există evaluări
- NSG-430 EcgDocument19 paginiNSG-430 EcgSarah RealÎncă nu există evaluări
- Gynecology MnemonicsDocument5 paginiGynecology MnemonicsJared Khoo Er HauÎncă nu există evaluări
- Neonatal Sepsis: CausesDocument3 paginiNeonatal Sepsis: CausesGeraldine BirowaÎncă nu există evaluări
- Case Simu 101Document5 paginiCase Simu 101Princess Levie CenizaÎncă nu există evaluări
- OB Care Plan: Assessment DataDocument9 paginiOB Care Plan: Assessment Dataapi-520841770Încă nu există evaluări
- Anesthesia Consent FormDocument2 paginiAnesthesia Consent Formbalab2311Încă nu există evaluări
- Transitional Care Case Study-Pulling It All TogetherDocument13 paginiTransitional Care Case Study-Pulling It All TogethermatthewÎncă nu există evaluări
- PPM Informed Consent in Anesthesia WITH FORMSDocument10 paginiPPM Informed Consent in Anesthesia WITH FORMSbalab2311Încă nu există evaluări
- CHN Clinical Rotation ExamDocument5 paginiCHN Clinical Rotation ExamAlvin JavierÎncă nu există evaluări
- nsg-432 Careplan 2Document11 pagininsg-432 Careplan 2api-521003884Încă nu există evaluări
- Kode SimpusDocument1 paginăKode SimpusRiky PratamaÎncă nu există evaluări
- Influenza VirusDocument17 paginiInfluenza Virusapi-458845511Încă nu există evaluări
- Health Teachings On CHFDocument6 paginiHealth Teachings On CHFfLOR_ZIANE_MAEÎncă nu există evaluări
- BS CareplanDocument11 paginiBS CareplanJulia BrownÎncă nu există evaluări
- Community Health Nursing Lecture: Family Health AssessmentDocument7 paginiCommunity Health Nursing Lecture: Family Health AssessmentSofia ResolÎncă nu există evaluări
- College of Nursing: Assessment Diagnosis Analysis Planning Implementation Rationale EvaluationDocument2 paginiCollege of Nursing: Assessment Diagnosis Analysis Planning Implementation Rationale EvaluationjoanneÎncă nu există evaluări
- Case Study 1: Nicole: 1. Discuss The Significance of Nicole's Laboratory FindingsDocument12 paginiCase Study 1: Nicole: 1. Discuss The Significance of Nicole's Laboratory FindingsClint NavarroÎncă nu există evaluări
- Case Simulatio 115Document6 paginiCase Simulatio 115Dudong SasakiÎncă nu există evaluări
- VSim Pharm (Mary Richards)Document3 paginiVSim Pharm (Mary Richards)Jay Blastic's arts and FunÎncă nu există evaluări
- Case Study, Chapter 70, Management of Patients WithOncologic or Degenerative Neurologic DisordersDocument1 paginăCase Study, Chapter 70, Management of Patients WithOncologic or Degenerative Neurologic Disordersclyde i am100% (1)
- PEDIA CASE 3 FinalDocument9 paginiPEDIA CASE 3 FinalXandra BnnÎncă nu există evaluări
- Nursing Process Overview: Health Assessment NotesDocument40 paginiNursing Process Overview: Health Assessment NotesEliakim III InsongÎncă nu există evaluări
- Assessment Diagnosis Inference Planning Intervention Rationale Outcomes Subjective DataDocument2 paginiAssessment Diagnosis Inference Planning Intervention Rationale Outcomes Subjective DataJoan GuisicÎncă nu există evaluări
- Kayla Flaskerud Vsim BP Concept Map, Isbar, ClincialDocument12 paginiKayla Flaskerud Vsim BP Concept Map, Isbar, ClincialCameron Janzen100% (1)
- Electrolyte ImbalanceDocument4 paginiElectrolyte ImbalanceDoneva Lyn MedinaÎncă nu există evaluări
- Vasquez - RLE A3 - PCCR (OSMUN Ward)Document16 paginiVasquez - RLE A3 - PCCR (OSMUN Ward)Mari Sheanne M. Vasquez100% (1)
- CERTIFIED NURSINGS ASSISTANT!!!!! Temperature Pulse and RespirationDocument28 paginiCERTIFIED NURSINGS ASSISTANT!!!!! Temperature Pulse and RespirationJonas VargasÎncă nu există evaluări
- Dhan Chan NCPDocument3 paginiDhan Chan NCPDhaneanne Marie ChanÎncă nu există evaluări
- Nursing Case Study - With Final Slides.Document77 paginiNursing Case Study - With Final Slides.veejai_kumar100% (2)
- Rle Neonate DrugsDocument13 paginiRle Neonate DrugsLhara Vhaneza CuetoÎncă nu există evaluări
- Teaching Plan For Hypertension - QHDocument2 paginiTeaching Plan For Hypertension - QHpamela_santiago_9100% (1)
- Cardiac NSG DiagnosisDocument5 paginiCardiac NSG DiagnosisShreyas WalvekarÎncă nu există evaluări
- Obstetric Nursing Care PlanDocument12 paginiObstetric Nursing Care PlanJass Mira Bueno100% (1)
- Final Teaching PlanDocument2 paginiFinal Teaching Planapi-352581650Încă nu există evaluări
- The Neonate at 24 To 48 Hours Following Early DischargeDocument8 paginiThe Neonate at 24 To 48 Hours Following Early Dischargenursereview100% (2)
- Clinical Learning ContractDocument3 paginiClinical Learning ContractKaragire vedasteÎncă nu există evaluări
- SBAR Communication Tool and Progress NoteDocument2 paginiSBAR Communication Tool and Progress Notejrj1111100% (1)
- Case Study 7Document29 paginiCase Study 7Hanniel MontecalboÎncă nu există evaluări
- Case Study #1 ScenarioDocument12 paginiCase Study #1 ScenarioHMG TVÎncă nu există evaluări
- Nursing Care Plan for Subarachnoid HemorrhageDocument46 paginiNursing Care Plan for Subarachnoid HemorrhageShitaljit IromÎncă nu există evaluări
- Beta ThalaDocument2 paginiBeta ThalaAngie LamoÎncă nu există evaluări
- Seizure Disorders in ChildrenDocument22 paginiSeizure Disorders in ChildrenBheru LalÎncă nu există evaluări
- Early Aggressive Nutrition Improves Growth in Premature InfantsDocument5 paginiEarly Aggressive Nutrition Improves Growth in Premature InfantsFlaming NbÎncă nu există evaluări
- South University College of Nursing Nursing Process Worksheet STUDENT: - Erica Clipps - NSG 3038 - FACULTY - Baby PlaceDocument3 paginiSouth University College of Nursing Nursing Process Worksheet STUDENT: - Erica Clipps - NSG 3038 - FACULTY - Baby PlaceErica ClippsÎncă nu există evaluări
- Teerthanker Mahaveer College of Nursing: BATCH-2019-2021Document32 paginiTeerthanker Mahaveer College of Nursing: BATCH-2019-2021Prasann RoyÎncă nu există evaluări
- Concept MapDocument1 paginăConcept Mapapi-246466200Încă nu există evaluări
- PoliomyelitisDocument4 paginiPoliomyelitisGerard Adad Misa100% (1)
- DVT Case StudyDocument2 paginiDVT Case StudyCrystal B Costa78Încă nu există evaluări
- CasestudyutiDocument21 paginiCasestudyutidael_05Încă nu există evaluări
- NCP Knowledge DeficitDocument2 paginiNCP Knowledge DeficitRainier IbarretaÎncă nu există evaluări
- Care of Adults 26 Endocrine ManagementDocument26 paginiCare of Adults 26 Endocrine ManagementGaras AnnaBerniceÎncă nu există evaluări
- Persuasive Communication in NursingDocument4 paginiPersuasive Communication in NursingNicole Audrey JoaquinÎncă nu există evaluări
- Pediatric Concept MapDocument12 paginiPediatric Concept Mapapi-352157080Încă nu există evaluări
- Waiters Newborn Care PDFDocument1 paginăWaiters Newborn Care PDFmp1757Încă nu există evaluări
- CPRDocument1 paginăCPRjanet roosevelt100% (1)
- Action Plan PICU FINALDocument2 paginiAction Plan PICU FINALMark MacasadduÎncă nu există evaluări
- Focus Charting in Pedia WardDocument32 paginiFocus Charting in Pedia Ward2A - Nicole Marrie HonradoÎncă nu există evaluări
- Neonatal Jaundice Case Study: Early Diagnosis and Treatment Prevents Brain DamageDocument6 paginiNeonatal Jaundice Case Study: Early Diagnosis and Treatment Prevents Brain DamagemuzamirÎncă nu există evaluări
- Ramos-2bn NCP Delivery RoomDocument2 paginiRamos-2bn NCP Delivery RoomLouwella RamosÎncă nu există evaluări
- NURSING CARE OF ADULTS II: Passbooks Study GuideDe la EverandNURSING CARE OF ADULTS II: Passbooks Study GuideÎncă nu există evaluări
- Building Blocks Issue 7 26 1Document10 paginiBuilding Blocks Issue 7 26 1balab2311Încă nu există evaluări
- Exercise For Persons With Cardiovascular DiseaseDocument3 paginiExercise For Persons With Cardiovascular Diseasebalab2311Încă nu există evaluări
- Azhaar TopicDocument4 paginiAzhaar Topicbalab2311Încă nu există evaluări
- Craniosynostosis & Craniofacial Surgery: A Parent's GuideDocument16 paginiCraniosynostosis & Craniofacial Surgery: A Parent's Guidebalab2311Încă nu există evaluări
- IndianJAnaesth542116-1332734 034207Document5 paginiIndianJAnaesth542116-1332734 034207balab2311Încă nu există evaluări
- InTech-Skull Expansion by Spring Mediated Bone RegenerationDocument27 paginiInTech-Skull Expansion by Spring Mediated Bone Regenerationbalab2311Încă nu există evaluări
- Neuro Hammer Ramamurthi RyanDocument3 paginiNeuro Hammer Ramamurthi Ryanbalab2311Încă nu există evaluări
- Midfacial Reconstruction Using Calvarial Split Bone GraftsDocument6 paginiMidfacial Reconstruction Using Calvarial Split Bone Graftsbalab2311Încă nu există evaluări
- Posterior Cranial Vault Distraction White 2009Document6 paginiPosterior Cranial Vault Distraction White 2009balab2311Încă nu există evaluări
- Read Ip LastDocument2 paginiRead Ip Lastbalab2311Încă nu există evaluări
- Onlay Bone Grafts Improve Coronal Synostosis CorrectionDocument9 paginiOnlay Bone Grafts Improve Coronal Synostosis Correctionbalab2311Încă nu există evaluări
- Midfacial Reconstruction Using Calvarial Split Bone GraftsDocument6 paginiMidfacial Reconstruction Using Calvarial Split Bone Graftsbalab2311Încă nu există evaluări
- 26 3 MovahedDocument4 pagini26 3 Movahedbalab2311Încă nu există evaluări
- 360 CheckDocument1 pagină360 Checkvishal821Încă nu există evaluări
- Particularities in The Surgical Technique of Calvaria GraftDocument6 paginiParticularities in The Surgical Technique of Calvaria Graftbalab2311Încă nu există evaluări
- Durable Grey Plaster for Walls and CeilingsDocument2 paginiDurable Grey Plaster for Walls and Ceilingsbalab2311Încă nu există evaluări
- Xtra Lite (AAC BLOCKS)Document2 paginiXtra Lite (AAC BLOCKS)Ektha RockyÎncă nu există evaluări
- PDF 10 Bonnes Raisons AnglaisDocument2 paginiPDF 10 Bonnes Raisons Anglaiscarumu01Încă nu există evaluări
- Concure LP90Document4 paginiConcure LP90balab2311Încă nu există evaluări
- Basic of Bone GraftingDocument29 paginiBasic of Bone GraftingdoctorniravÎncă nu există evaluări
- KaushikresumeDocument3 paginiKaushikresumebalab2311Încă nu există evaluări
- 2509datasheetconcure LP90Document2 pagini2509datasheetconcure LP90balab2311Încă nu există evaluări
- AspirationDocument1 paginăAspirationbalab2311Încă nu există evaluări
- Concure WBDocument3 paginiConcure WBbalab2311Încă nu există evaluări
- Anesthesia Consent 1 PDFDocument2 paginiAnesthesia Consent 1 PDFbalab2311Încă nu există evaluări
- Information For Authors PDFDocument4 paginiInformation For Authors PDFbalab2311Încă nu există evaluări
- RIMS THESIS TOPICS ON GALLSTONES AND APPENDICITISDocument3 paginiRIMS THESIS TOPICS ON GALLSTONES AND APPENDICITISroshansanasamÎncă nu există evaluări
- Newborn Admission Under 40 CharactersDocument2 paginiNewborn Admission Under 40 CharactersonijinoÎncă nu există evaluări
- HYDROCELEDocument12 paginiHYDROCELEChristin Feliana SitanggangÎncă nu există evaluări
- Sketchy TrackerDocument36 paginiSketchy Trackerpsy killÎncă nu există evaluări
- Symptoms of Diabetes: Losing Weight and Keeping It OffDocument10 paginiSymptoms of Diabetes: Losing Weight and Keeping It OffGohar imranÎncă nu există evaluări
- Diagnosa Banding PneumoniaDocument7 paginiDiagnosa Banding PneumoniaLuphly TaluvtaÎncă nu există evaluări
- Postnatal LeafletDocument2 paginiPostnatal LeafletAnonymous miY5zfHÎncă nu există evaluări
- What Is AsthmaDocument4 paginiWhat Is AsthmaGarimaBhayanaÎncă nu există evaluări
- Human Papilloma VirusDocument21 paginiHuman Papilloma VirusVasuda Devi MalepatiÎncă nu există evaluări
- CEFUROXIMEDocument1 paginăCEFUROXIMEJose Luis HernandezÎncă nu există evaluări
- EUCAST System For Antimicrobial Abbreviations: Method For Selection of A Unique Three-Letter CodeDocument2 paginiEUCAST System For Antimicrobial Abbreviations: Method For Selection of A Unique Three-Letter CodeMarcelo UGÎncă nu există evaluări
- Dr. Firdha's Morning Report on ER Patient with CKD, HF & CAPDocument4 paginiDr. Firdha's Morning Report on ER Patient with CKD, HF & CAPFirdha RositaÎncă nu există evaluări
- Pengaruh Massage Kaki Terhadap Penurunan Insomnia Pada Lansia Di Banjar Temesi Desa Temesi Kabupaten GianyarDocument12 paginiPengaruh Massage Kaki Terhadap Penurunan Insomnia Pada Lansia Di Banjar Temesi Desa Temesi Kabupaten Gianyar119 CIKOKOLÎncă nu există evaluări
- Respiratory System Pharmacology NotesDocument15 paginiRespiratory System Pharmacology NotesAli Rahimi100% (1)
- OB/GYN For EMS ProvidersDocument94 paginiOB/GYN For EMS ProvidersPaulhotvw67100% (6)
- Nursing exam covers hypertension, anemia, surgeryDocument8 paginiNursing exam covers hypertension, anemia, surgeryBurhan uddin100% (2)
- Abdominal Pain DischargeDocument2 paginiAbdominal Pain Dischargemfa40Încă nu există evaluări
- Rush Breast Surgeons Patient Intake FormDocument3 paginiRush Breast Surgeons Patient Intake FormVijungcoÎncă nu există evaluări
- Peptic Ulcer DiseaseDocument8 paginiPeptic Ulcer Diseasepragna novaÎncă nu există evaluări
- What Are The Symptoms Measles (Focus On Measles More, Then Talk About Mumps and Rubella)Document2 paginiWhat Are The Symptoms Measles (Focus On Measles More, Then Talk About Mumps and Rubella)RexDavidGidoÎncă nu există evaluări
- Medicamentos genéricos y de marca con preciosDocument46 paginiMedicamentos genéricos y de marca con preciosscribdlawrnceÎncă nu există evaluări
- Fever Cheat Sheet Information Graphic Todays Parent Braun 1Document1 paginăFever Cheat Sheet Information Graphic Todays Parent Braun 1canmyutÎncă nu există evaluări