S-ar putea să vă placă și
- Dentists: What You Need to Know Before Choosing a DentistDe la EverandDentists: What You Need to Know Before Choosing a DentistÎncă nu există evaluări
- Medical Equipment and Supply Business: Your Multi Billion Dollar Guide to Start-UpDe la EverandMedical Equipment and Supply Business: Your Multi Billion Dollar Guide to Start-UpÎncă nu există evaluări
- Benefits Overview 2018Document5 paginiBenefits Overview 2018Joby JoÎncă nu există evaluări
- Geaso Parental Health Plan Brochure - REVISED 2020Document2 paginiGeaso Parental Health Plan Brochure - REVISED 2020shanesmdÎncă nu există evaluări
- Standard Schedule of Benefits - Market Street LTD 2022Document2 paginiStandard Schedule of Benefits - Market Street LTD 2022mariojesus8807Încă nu există evaluări
- CLICO Group Health and Life Coverage 1Document12 paginiCLICO Group Health and Life Coverage 1buckianÎncă nu există evaluări
- Cardea Schedule of Benefits Effective Jan 1st 2021Document4 paginiCardea Schedule of Benefits Effective Jan 1st 2021Wayne GajadharÎncă nu există evaluări
- Lawe Silver BrochureDocument6 paginiLawe Silver BrochureLavinea SmithÎncă nu există evaluări
- Dental Plan Side-By-Side Comparison: Fast FactsDocument2 paginiDental Plan Side-By-Side Comparison: Fast FactsellenÎncă nu există evaluări
- Lewermark Health Insurance Copay Plan For Delta State UniversityDocument3 paginiLewermark Health Insurance Copay Plan For Delta State Universityroby sorianoÎncă nu există evaluări
- SafeTravels Visitors PDFDocument21 paginiSafeTravels Visitors PDFpisharmaÎncă nu există evaluări
- Your Customized Benefits Plan at HCL America IncDocument2 paginiYour Customized Benefits Plan at HCL America IncShiv RanjanÎncă nu există evaluări
- Benefit at A GlanceDocument2 paginiBenefit at A GlanceShiv ChauhanÎncă nu există evaluări
- Brochure PDF MANHATTHAN LIFEDocument2 paginiBrochure PDF MANHATTHAN LIFEEmanuel ChirinosÎncă nu există evaluări
- Compass: Gold / SilverDocument16 paginiCompass: Gold / SilverStan SmithÎncă nu există evaluări
- Snap Guardian Dental Plan Summary 2022Document4 paginiSnap Guardian Dental Plan Summary 2022Samson FungÎncă nu există evaluări
- Benefits HighlightsDocument1 paginăBenefits HighlightsRobert AvramescuÎncă nu există evaluări
- De Luxe0607Document7 paginiDe Luxe0607tewary_rahulÎncă nu există evaluări
- 2010 UnitedHealthcare Benefits SummaryDocument1 pagină2010 UnitedHealthcare Benefits Summaryapi-27017317Încă nu există evaluări
- CAMAF Benefit Brochure 2014Document2 paginiCAMAF Benefit Brochure 20140796105632Încă nu există evaluări
- 2023 FMCNA Medical Plan Cost ComparisonDocument2 pagini2023 FMCNA Medical Plan Cost ComparisonCristal PeoplesÎncă nu există evaluări
- USS Pre-Medicare PPO With RX PlanDocument3 paginiUSS Pre-Medicare PPO With RX PlanAnonymous w0egAgMouGÎncă nu există evaluări
- Summary of 2022 Benefit Changes: MedicalDocument5 paginiSummary of 2022 Benefit Changes: MedicalChinnu SalimathÎncă nu există evaluări
- Schedule of Benefits (Enhanced Silver Plan With Dental & Optical)Document3 paginiSchedule of Benefits (Enhanced Silver Plan With Dental & Optical)kishan310Încă nu există evaluări
- Generic Open Enrollment KitDocument22 paginiGeneric Open Enrollment KitSteve BarrowsÎncă nu există evaluări
- Pet Insurance ComparisonsDocument2 paginiPet Insurance ComparisonsHSVC50% (2)
- Photon Benefits 2022 (August)Document7 paginiPhoton Benefits 2022 (August)sojithesouljaÎncă nu există evaluări
- Protect What You Treasure Most: HealthDocument12 paginiProtect What You Treasure Most: HealthNelly HÎncă nu există evaluări
- BCBS Enrollment GuideDocument6 paginiBCBS Enrollment GuideAnonymous Lri40PrlkÎncă nu există evaluări
- Benefits Highlights 2018Document5 paginiBenefits Highlights 2018Marcus CosmeÎncă nu există evaluări
- PruBSN Medic Protector Brochure ENGDocument12 paginiPruBSN Medic Protector Brochure ENGseefengshuiÎncă nu există evaluări
- Isoa Hea OMPASS - 2016 - 2017 PDFDocument13 paginiIsoa Hea OMPASS - 2016 - 2017 PDFSharif M Mizanur RahmanÎncă nu există evaluări
- Medical Comparison Chart 2020Document3 paginiMedical Comparison Chart 2020hollingermikeÎncă nu există evaluări
- Kaiser Permanente Compare Plans CA 2011 KPIFDocument1 paginăKaiser Permanente Compare Plans CA 2011 KPIFDennis AlexanderÎncă nu există evaluări
- Young Adult BrochureDocument5 paginiYoung Adult BrochureahsanÎncă nu există evaluări
- Group Critical Illness Insurance CoverageDocument2 paginiGroup Critical Illness Insurance CoverageAndrewÎncă nu există evaluări
- Enhanced Healthcare SchemesDocument2 paginiEnhanced Healthcare SchemesSyed ZaheedÎncă nu există evaluări
- 2 VEBA Plan ComparisonDocument2 pagini2 VEBA Plan ComparisonMitchell BigleyÎncă nu există evaluări
- Blue ChoiceDocument5 paginiBlue ChoiceahsanÎncă nu există evaluări
- ConvertDocument2 paginiConvertpham_thu_hangÎncă nu există evaluări
- Eb 2019 Oe Guideplussbc GenericDocument19 paginiEb 2019 Oe Guideplussbc GenericCybernaughtÎncă nu există evaluări
- HOMEOWNERS PROTECTION PLAN HPP Superior PlanDocument11 paginiHOMEOWNERS PROTECTION PLAN HPP Superior PlanJose Antonio ReyesÎncă nu există evaluări
- Vanderbilt phf-21-22Document2 paginiVanderbilt phf-21-22api-458468763Încă nu există evaluări
- 2020 Ankura Benefits GuideDocument20 pagini2020 Ankura Benefits GuidegpperkÎncă nu există evaluări
- HPA00001134392 Mansfield PAC 3557 HP 1625 Coverage Selection FormDocument7 paginiHPA00001134392 Mansfield PAC 3557 HP 1625 Coverage Selection FormLinda MansfieldÎncă nu există evaluări
- Health & Dental Handout JUN17Document2 paginiHealth & Dental Handout JUN17Darius YangÎncă nu există evaluări
- I-Great Evo - Female 2Document1 paginăI-Great Evo - Female 2Fuad ShakirÎncă nu există evaluări
- Cash Plan 100 Table+of+coverDocument8 paginiCash Plan 100 Table+of+covermuthukumaran.tdr2969Încă nu există evaluări
- Medical RealDocument1 paginăMedical Realapi-252555369Încă nu există evaluări
- Copy of 2020 ID List of Benefits and Allowances ARZxlsx - 2. Medical Insurance UpdDocument1 paginăCopy of 2020 ID List of Benefits and Allowances ARZxlsx - 2. Medical Insurance Updfrututu.smoothiesÎncă nu există evaluări
- Unitedhealthcare Dental Ppo Plan 2022 Summary of Benefits and CoverageDocument1 paginăUnitedhealthcare Dental Ppo Plan 2022 Summary of Benefits and CoverageAdam CliftonÎncă nu există evaluări
- VIC BrochureDocument8 paginiVIC BrochureArnab AcharyaÎncă nu există evaluări
- 2022 Benefits Summary For FA EE'sDocument6 pagini2022 Benefits Summary For FA EE'sFrancisca VigilÎncă nu există evaluări
- Senior Citizens Red Carpet Health Insurance Policy PDFDocument8 paginiSenior Citizens Red Carpet Health Insurance Policy PDFrohit22221Încă nu există evaluări
- JACAM Benefit OverviewDocument7 paginiJACAM Benefit OverviewStephenDohertyÎncă nu există evaluări
- Manulife CoverMe FollowMe Health Comp Chart Jan 2018 ENGLISHDocument2 paginiManulife CoverMe FollowMe Health Comp Chart Jan 2018 ENGLISHMamacintÎncă nu există evaluări
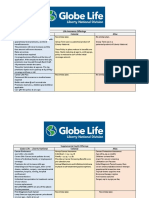
- Life Insurance Offerings Globe Life - Liberty National Colonial AflacDocument3 paginiLife Insurance Offerings Globe Life - Liberty National Colonial AflacTina Hughes0% (1)
- FHO, CHI, WC, ASSURE, Coparison One PagerDocument1 paginăFHO, CHI, WC, ASSURE, Coparison One PagerLakshmikanth SÎncă nu există evaluări
- Schedule of Benefits (Core Silver Without Dental)Document3 paginiSchedule of Benefits (Core Silver Without Dental)Afkar inteÎncă nu există evaluări
- Guardian Life of The CaribbeanDocument1 paginăGuardian Life of The CaribbeanKammieÎncă nu există evaluări
- Barbados Budgetary Proposal 2010 AddendumDocument2 paginiBarbados Budgetary Proposal 2010 AddendumKammieÎncă nu există evaluări
- Accountabilty and Offering Excuses For ExcusesDocument1 paginăAccountabilty and Offering Excuses For ExcusesKammieÎncă nu există evaluări
- CoopMED Health Insurance Doctor Examination FormDocument2 paginiCoopMED Health Insurance Doctor Examination FormKammieÎncă nu există evaluări
- Barbados Affordable Critical Care InsuranceDocument1 paginăBarbados Affordable Critical Care InsuranceKammieÎncă nu există evaluări
- Barbados Budgetary Proposal 2010Document228 paginiBarbados Budgetary Proposal 2010KammieÎncă nu există evaluări
- EzineDocument2 paginiEzineKammieÎncă nu există evaluări
- Guardian Holdings PM David ThompsonDocument1 paginăGuardian Holdings PM David ThompsonKammieÎncă nu există evaluări
- Barbados Guardian General Home Insurance Online Quotation FormDocument1 paginăBarbados Guardian General Home Insurance Online Quotation FormKammieÎncă nu există evaluări
- Why Waste Your Waste - Antigua - KammieDocument29 paginiWhy Waste Your Waste - Antigua - KammieKammie100% (1)
- Barbados Credit Unions CoopMED Medical Health InsuranceDocument4 paginiBarbados Credit Unions CoopMED Medical Health InsuranceKammieÎncă nu există evaluări
- Guardian General Vehicle Insurance Quotation Form OnlineDocument1 paginăGuardian General Vehicle Insurance Quotation Form OnlineKammieÎncă nu există evaluări
- Barbados Credit Unions Funeral InsuranceDocument12 paginiBarbados Credit Unions Funeral InsuranceKammieÎncă nu există evaluări
- Is There Something Made by Man That Approaches The Beauty of Nature? Perhaps Music!Document44 paginiIs There Something Made by Man That Approaches The Beauty of Nature? Perhaps Music!Grizzly GroundswellÎncă nu există evaluări
- Barbados Credit Unions CoopMED Affordable Medical InsuranceDocument15 paginiBarbados Credit Unions CoopMED Affordable Medical InsuranceKammieÎncă nu există evaluări
- Barbados NemCare Insurance Small Groups DataDocument2 paginiBarbados NemCare Insurance Small Groups DataKammieÎncă nu există evaluări
- Barbados NemCare Health Insurance Census Data Quotation FormDocument18 paginiBarbados NemCare Health Insurance Census Data Quotation FormKammieÎncă nu există evaluări
- Demographic Change FormDocument2 paginiDemographic Change FormKammieÎncă nu există evaluări
- Spin SellingDocument45 paginiSpin SellingKammie100% (15)
- Application CoopMED Health Insurance Plan BarbadosDocument2 paginiApplication CoopMED Health Insurance Plan BarbadosKammieÎncă nu există evaluări
- Barbados Co-opLIFE Credit Union Funeral InsuranceDocument11 paginiBarbados Co-opLIFE Credit Union Funeral InsuranceKammie100% (1)
- Herpes Simplex PDFDocument28 paginiHerpes Simplex PDFAnggi Tridinanti PutriÎncă nu există evaluări
- Atod Practice QuizDocument1 paginăAtod Practice Quizapi-263456844100% (1)
- A Date With DestinyDocument27 paginiA Date With DestinyJayvee Fulgencio100% (2)
- 15 Foods That Fight Prostate CancerDocument2 pagini15 Foods That Fight Prostate CancerArt100% (1)
- Haematology Practice MCQsDocument3 paginiHaematology Practice MCQsmonday125100% (1)
- Scored Patient Generated Subjective Global Assessment PG SGA PDFDocument2 paginiScored Patient Generated Subjective Global Assessment PG SGA PDFOrlea Francisco-Sisio100% (1)
- Properties: Edibility / CulinaryDocument6 paginiProperties: Edibility / CulinaryHershey Flores RemolonaÎncă nu există evaluări
- Maur MeyerDocument488 paginiMaur MeyerItachi KunÎncă nu există evaluări
- TEST BANK For The Language of Medicine 12th Edition by Chabner Chapter 1 - 21 CompleteDocument28 paginiTEST BANK For The Language of Medicine 12th Edition by Chabner Chapter 1 - 21 Completemarcuskenyatta275Încă nu există evaluări
- Onco Intensive Nursing ReviewerDocument14 paginiOnco Intensive Nursing ReviewerAllysa PrestonÎncă nu există evaluări
- Lettre de Hollingsworth À Consolato Maria SergiDocument6 paginiLettre de Hollingsworth À Consolato Maria SergiLeMonde.frÎncă nu există evaluări
- New Microsoft Word DocdfumentDocument15 paginiNew Microsoft Word DocdfumentHE141358 Tran Vu Khanh Duy100% (1)
- Colorectal AdenocarcinomaDocument48 paginiColorectal Adenocarcinomamingchuan chuÎncă nu există evaluări
- The World Health Organization Three-Step Analgesic LadderDocument2 paginiThe World Health Organization Three-Step Analgesic LadderRisti FishyÎncă nu există evaluări
- Health Assessment Handout MayannDocument9 paginiHealth Assessment Handout MayannDENNIS N. MUÑOZÎncă nu există evaluări
- 4 Lab ManualDocument160 pagini4 Lab ManualAziz EzoÎncă nu există evaluări
- Medsave Request For Pre Authorisation FormDocument2 paginiMedsave Request For Pre Authorisation FormM/s MicrotechÎncă nu există evaluări
- Antihistamine Bilastine A Novel Antihistamine 2018Document4 paginiAntihistamine Bilastine A Novel Antihistamine 2018SRINIVASÎncă nu există evaluări
- DohDocument8 paginiDohJai MacanasÎncă nu există evaluări
- ICCR Lung 4th Ed v4.0 HyperlinkDocument5 paginiICCR Lung 4th Ed v4.0 HyperlinkOlteanu Gheorghe-EmilianÎncă nu există evaluări
- Tepotinib in Non-Small-Cell Lung Cancer With MET Exon 14 Skipping Mutations JCDocument4 paginiTepotinib in Non-Small-Cell Lung Cancer With MET Exon 14 Skipping Mutations JCYaramÎncă nu există evaluări
- Susah BabDocument45 paginiSusah BabaghniaÎncă nu există evaluări
- Anal Fissures & FistulasDocument3 paginiAnal Fissures & FistulasLouis FortunatoÎncă nu există evaluări
- Hartmann Procedure - Google SearchDocument1 paginăHartmann Procedure - Google SearchGrizzel CortesÎncă nu există evaluări
- Intl Journal of Cancer - 2024 - Oyelere - Coffee Consumption Is Associated With A Reduced Risk of Colorectal CancerDocument10 paginiIntl Journal of Cancer - 2024 - Oyelere - Coffee Consumption Is Associated With A Reduced Risk of Colorectal CancerRoel PlmrsÎncă nu există evaluări
- Examining The PrecordiumDocument83 paginiExamining The PrecordiumnicolÎncă nu există evaluări
- Hifema: Dr. Bobi Ahmad Sahid, S.KepDocument21 paginiHifema: Dr. Bobi Ahmad Sahid, S.Kepdr.Bobi Ahmad Sahid, S.KepÎncă nu există evaluări
- PI MaltoferDocument15 paginiPI MaltoferrazhossenÎncă nu există evaluări
- Nursing DiagnosisDocument4 paginiNursing Diagnosiskendralyn0212408233% (3)
- Treatment of Glioblastoma With Herbal MedicinesDocument14 paginiTreatment of Glioblastoma With Herbal MedicinesGabrielAbarcaÎncă nu există evaluări