S-ar putea să vă placă și
- AmoebiasisDocument5 paginiAmoebiasisyondaime268875Încă nu există evaluări
- Entamoeba HistolyticaDocument10 paginiEntamoeba HistolyticaMin-Joo Esther ParkÎncă nu există evaluări
- Case Study of AmoebiasisDocument7 paginiCase Study of Amoebiasisbuzz Q75% (4)
- IntroductionDocument6 paginiIntroductionAnne RiztiaÎncă nu există evaluări
- Case Study of AmoebiasisDocument16 paginiCase Study of AmoebiasisGlorielle ElvambuenaÎncă nu există evaluări
- Intestinal 0 Amphizoic Amoebae Sikatema Mike PDFDocument37 paginiIntestinal 0 Amphizoic Amoebae Sikatema Mike PDFbrainworxeducationÎncă nu există evaluări
- Intestinal and Amphizoic Amoeba M SikatemaDocument70 paginiIntestinal and Amphizoic Amoeba M SikatemabrainworxeducationÎncă nu există evaluări
- Amoeba Notes 2015Document6 paginiAmoeba Notes 2015Ivy FlorentinoÎncă nu există evaluări
- Amoebiasis and AmoebaDocument10 paginiAmoebiasis and AmoebaStephanie Joy EscalaÎncă nu există evaluări
- Belizario ParasitologyDocument66 paginiBelizario Parasitologyangela tanteoÎncă nu există evaluări
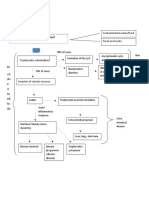
- Amoebiasis PathophysiologyDocument3 paginiAmoebiasis PathophysiologyApril CornejoÎncă nu există evaluări
- RP RPDocument6 paginiRP RPEliezah RodriguezÎncă nu există evaluări
- CD Learning Material 3 Water BorneDocument16 paginiCD Learning Material 3 Water BorneDaime ValdezÎncă nu există evaluări
- Protozoan Mmrs Intestinal ProtozoaDocument33 paginiProtozoan Mmrs Intestinal ProtozoabrainworxeducationÎncă nu există evaluări
- Oral Fecal Route Diseases Oral Fecal Route Diseases: Afroz Lakhani RN, BSCNDocument74 paginiOral Fecal Route Diseases Oral Fecal Route Diseases: Afroz Lakhani RN, BSCNafrozlakhaniÎncă nu există evaluări
- Entamoeba Histolytica (Medical Microbiology-Jawetz)Document20 paginiEntamoeba Histolytica (Medical Microbiology-Jawetz)manmithÎncă nu există evaluări
- AMOEBIASISDocument16 paginiAMOEBIASISAngeline TaghapÎncă nu există evaluări
- Human Digestive SystemDocument5 paginiHuman Digestive SystemPau BurceÎncă nu există evaluări
- Acute Diarrhoea and VomitingDocument43 paginiAcute Diarrhoea and VomitingAdriana AfiqahÎncă nu există evaluări
- Intestinal Pathogens: Department of Clinical Microbiology Medical Faculty Universitas BrawijayaDocument56 paginiIntestinal Pathogens: Department of Clinical Microbiology Medical Faculty Universitas BrawijayaPipitÎncă nu există evaluări
- Amebiasis and Schistosomiasis OutlineDocument14 paginiAmebiasis and Schistosomiasis OutlineAldave MoonÎncă nu există evaluări
- Plenary 3 Group 13Document122 paginiPlenary 3 Group 13Obet Agung 天Încă nu există evaluări
- Lesson 3 Amoebiasis: Entamoeba HistolyticaDocument7 paginiLesson 3 Amoebiasis: Entamoeba HistolyticaAstrid FausziaÎncă nu există evaluări
- Amoebic DysenteryDocument2 paginiAmoebic Dysenteryyuvi087Încă nu există evaluări
- AmoebiasisDocument3 paginiAmoebiasisKrista CabelloÎncă nu există evaluări
- Entamoeba Histolytica 3Document37 paginiEntamoeba Histolytica 3divelian johnÎncă nu există evaluări
- AMOEBIASISDocument1 paginăAMOEBIASISjeromedcÎncă nu există evaluări
- AMOEBIASISDocument8 paginiAMOEBIASISCheska ت HortelanoÎncă nu există evaluări
- Entameba HistolyticaDocument7 paginiEntameba HistolyticaDjdjjd SiisusÎncă nu există evaluări
- AmoebiasisDocument1 paginăAmoebiasisYakumaÎncă nu există evaluări
- Etiologi Dan Patofisiologi Bedah DigestifDocument46 paginiEtiologi Dan Patofisiologi Bedah DigestifNurul HidayatiÎncă nu există evaluări
- AmoebiasisDocument4 paginiAmoebiasisnamanÎncă nu există evaluări
- JHS Digestive SystemDocument35 paginiJHS Digestive SystemGojo KaisenÎncă nu există evaluări
- AMOEBIASISDocument5 paginiAMOEBIASISKavyarani RathodÎncă nu există evaluări
- Infeksi Protozoa Amebiasis: Ni Nyoman Sintya Agniswari Anasta Putri 1670121028 SGD 4Document9 paginiInfeksi Protozoa Amebiasis: Ni Nyoman Sintya Agniswari Anasta Putri 1670121028 SGD 4sintya agniswariÎncă nu există evaluări
- AmebiasisDocument14 paginiAmebiasisxxxchi chaxxxÎncă nu există evaluări
- Crohn's Disease - CSDocument28 paginiCrohn's Disease - CSMASII100% (2)
- Digestive System Lecture NotesdocxDocument11 paginiDigestive System Lecture NotesdocxAdaÎncă nu există evaluări
- Differential Diagnosis: Disease/Condition Differentiating Signs/Symptoms Differentiating TestsDocument3 paginiDifferential Diagnosis: Disease/Condition Differentiating Signs/Symptoms Differentiating TestsJim Christian EllaserÎncă nu există evaluări
- Case 1Document11 paginiCase 1Gwendolyn Talahiban LusaraÎncă nu există evaluări
- Anatomy and Physiology 1&2 (Part 3)Document124 paginiAnatomy and Physiology 1&2 (Part 3)Kleindyn Joy PeraltaÎncă nu există evaluări
- Amoeb Iasis: By: Sytrose Morales TabacoDocument13 paginiAmoeb Iasis: By: Sytrose Morales TabacoSytrose MoralesÎncă nu există evaluări
- AmoebiasisDocument34 paginiAmoebiasisFevie Marie Aguilar67% (3)
- Sic 2Document4 paginiSic 2Ezra Miguel DarundayÎncă nu există evaluări
- Sarcomastigophora: A Phylum of PROTOZOA Subphyla: SARCODINA and Have Flagella or PseudopodiaDocument20 paginiSarcomastigophora: A Phylum of PROTOZOA Subphyla: SARCODINA and Have Flagella or Pseudopodiaabel semuÎncă nu există evaluări
- Gastroenteritis - Pathology & PhysiologyDocument1 paginăGastroenteritis - Pathology & PhysiologyKatie JusayÎncă nu există evaluări
- Pathogens of The Gut - Christine ProchnowDocument1 paginăPathogens of The Gut - Christine ProchnowMicroposterÎncă nu există evaluări
- Digestive: M4 CONSOLACION, Tristan M9 SANIDAD, Erwin F2 ALONZO, Roxanne F7 CARREON, CassandraDocument6 paginiDigestive: M4 CONSOLACION, Tristan M9 SANIDAD, Erwin F2 ALONZO, Roxanne F7 CARREON, CassandraTristan Tabago ConsolacionÎncă nu există evaluări
- Amoebiasis in Wild Mammals: Ayesha Ahmed M Phil. Parasitology 1 Semester 2013-Ag-2712Document25 paginiAmoebiasis in Wild Mammals: Ayesha Ahmed M Phil. Parasitology 1 Semester 2013-Ag-2712Abdullah AzeemÎncă nu există evaluări
- PROTOZOOLOGYDocument44 paginiPROTOZOOLOGYFanny Ross UrreaÎncă nu există evaluări
- M5 Post Task - AmoebiasisDocument1 paginăM5 Post Task - Amoebiasisbing bongÎncă nu există evaluări
- Parasitiology Semi ExamDocument26 paginiParasitiology Semi ExamHILVANO, HEIDEE B.Încă nu există evaluări
- Module 6Document26 paginiModule 6xtnreyesÎncă nu există evaluări
- AmoebiasisDocument14 paginiAmoebiasisPRATIK SHRESTHAÎncă nu există evaluări
- AmoebaeDocument80 paginiAmoebaemicroperadeniya0% (2)
- AmoebaDocument3 paginiAmoebaApril CornejoÎncă nu există evaluări
- G Lamblia: (Open Table in A New Window)Document6 paginiG Lamblia: (Open Table in A New Window)Ahmed Ben BellaÎncă nu există evaluări
- 4 Digestive Disorders of DogsDocument72 pagini4 Digestive Disorders of DogsKoleen Lopez ÜÎncă nu există evaluări
- Probiotic Rescue: How You can use Probiotics to Fight Cholesterol, Cancer, Superbugs, Digestive Complaints and MoreDe la EverandProbiotic Rescue: How You can use Probiotics to Fight Cholesterol, Cancer, Superbugs, Digestive Complaints and MoreÎncă nu există evaluări
- Nursing Care Plan: Assessment Diagnosis Planning Intervention Evaluation S: "Pabalik-Balik Pa IndependentDocument2 paginiNursing Care Plan: Assessment Diagnosis Planning Intervention Evaluation S: "Pabalik-Balik Pa IndependenthsiriaÎncă nu există evaluări
- Pa Tho PhysiologyDocument2 paginiPa Tho PhysiologyhsiriaÎncă nu există evaluări
- Salmonella Typhi (S. Typhi) - Common Worldwide, It Is Transmitted by The Fecal-Oral RouteDocument4 paginiSalmonella Typhi (S. Typhi) - Common Worldwide, It Is Transmitted by The Fecal-Oral Routehsiria100% (1)
- NCP-Drug Study 2Document4 paginiNCP-Drug Study 2hsiriaÎncă nu există evaluări
- A Case Study of PneumoniaDocument13 paginiA Case Study of PneumoniahsiriaÎncă nu există evaluări
- Patient's ProfileDocument1 paginăPatient's ProfilehsiriaÎncă nu există evaluări
- NCP 2Document2 paginiNCP 2hsiria100% (1)
- NCP 3Document3 paginiNCP 3hsiriaÎncă nu există evaluări
- NCP 1Document1 paginăNCP 1hsiriaÎncă nu există evaluări
- A Case Study of Hypertensive Cardiovascular Disease (HCVD) : School of Nursing and MidwiferyDocument13 paginiA Case Study of Hypertensive Cardiovascular Disease (HCVD) : School of Nursing and Midwiferyhsiria100% (2)
- NCPDocument6 paginiNCPhsiria100% (1)
- Drug StudyDocument4 paginiDrug StudyhsiriaÎncă nu există evaluări
- NCP 2Document2 paginiNCP 2hsiria100% (1)
- Nursing Care Plan: Assessment Nursing Diagnosis Scientific Explanation Planning Interventions Rationale EvaluationDocument2 paginiNursing Care Plan: Assessment Nursing Diagnosis Scientific Explanation Planning Interventions Rationale EvaluationhsiriaÎncă nu există evaluări
- Nursing Care Plan: Assessment Nursing Diagnosis Scientific Explanation Planning Interventions Rationale EvaluationDocument3 paginiNursing Care Plan: Assessment Nursing Diagnosis Scientific Explanation Planning Interventions Rationale EvaluationhsiriaÎncă nu există evaluări
- Histology of Esophagus For 2nd Year by DR SUNDUSDocument21 paginiHistology of Esophagus For 2nd Year by DR SUNDUSMudassar RoomiÎncă nu există evaluări
- NCERT - Exemplar - Life ProcessesDocument26 paginiNCERT - Exemplar - Life ProcessesRagini BaghelÎncă nu există evaluări
- THE Process of DigestionDocument39 paginiTHE Process of Digestionskaii100% (1)
- Cat Digestive SystemDocument7 paginiCat Digestive SystemPattyÎncă nu există evaluări
- Digestive System: Arba P. RamadaniDocument28 paginiDigestive System: Arba P. RamadaniQd Vella QnozesDanteÎncă nu există evaluări
- Frog Digestive SystemDocument10 paginiFrog Digestive SystemNatasha Mae ValdezÎncă nu există evaluări
- Your Wondrous Nervous System: Gunnar Backstrom, PHDDocument69 paginiYour Wondrous Nervous System: Gunnar Backstrom, PHDAlberto AlbertoÎncă nu există evaluări
- Topic:: Bixby Knolls Preparatory Academy - San Antonio, QuezonDocument3 paginiTopic:: Bixby Knolls Preparatory Academy - San Antonio, QuezonTeacher OliÎncă nu există evaluări
- Life ProcessDocument8 paginiLife ProcessKumar AbhishantÎncă nu există evaluări
- The General Anatomy of The Teeth Comparative Anatomy of The TeethDocument9 paginiThe General Anatomy of The Teeth Comparative Anatomy of The Teethsomebody_maÎncă nu există evaluări
- HCPro Inc., Adrianne E. Avillion DEd RN Reviewer ICD-10 Competency Assessment For Coders Anatomy and PhysiologyDocument54 paginiHCPro Inc., Adrianne E. Avillion DEd RN Reviewer ICD-10 Competency Assessment For Coders Anatomy and PhysiologyamruthkiranbabujiÎncă nu există evaluări
- Activity 10Document6 paginiActivity 10SeaÎncă nu există evaluări
- Visualizing Nutrition 3rd Edition by Mary B. - Test BankDocument51 paginiVisualizing Nutrition 3rd Edition by Mary B. - Test Bankroseyoung0Încă nu există evaluări
- Health Book For TeachersDocument281 paginiHealth Book For TeachersRene H. Framcisco, MD100% (2)
- Course Syllabus in Science VIII: Marcelino Fule Memorial College Alaminos, Laguna S.Y. 2020-2021Document8 paginiCourse Syllabus in Science VIII: Marcelino Fule Memorial College Alaminos, Laguna S.Y. 2020-2021Lhaine F.Încă nu există evaluări
- Repaso 1 Natural ScienceDocument8 paginiRepaso 1 Natural ScienceElenaÎncă nu există evaluări
- Sistem Pencernaan RuminansiaDocument37 paginiSistem Pencernaan RuminansiaIndah Fitri Sakinah LimbongÎncă nu există evaluări
- Interior Root WordsDocument3 paginiInterior Root WordsPaula McAuliffeÎncă nu există evaluări
- Digestive System and Parts Function: 12STEM-1 General Biology 2Document4 paginiDigestive System and Parts Function: 12STEM-1 General Biology 2hazel lagaticÎncă nu există evaluări
- Chemistry ProjectDocument12 paginiChemistry ProjectCricket ClutchÎncă nu există evaluări
- Quiz Bee ScienceDocument2 paginiQuiz Bee ScienceAndrew Bondad88% (8)
- Calculous Cholecystitis Case Study SampleDocument137 paginiCalculous Cholecystitis Case Study SampleKatie Lacuata80% (5)
- Mechanical and Chemical Digestion in The Mouth - Hussain Ali HamdanDocument4 paginiMechanical and Chemical Digestion in The Mouth - Hussain Ali HamdanHussain Ali AlkinanyÎncă nu există evaluări
- Class7 Science Unit02 NCERTDocument13 paginiClass7 Science Unit02 NCERTManoj Kumar TewariÎncă nu există evaluări
- Digestion Enzyme Practice TestDocument15 paginiDigestion Enzyme Practice TestJila HafiziÎncă nu există evaluări
- 15 Health Benefits of Radish, According To Science (+6 Delicious Recipes)Document23 pagini15 Health Benefits of Radish, According To Science (+6 Delicious Recipes)Nandan AcharyaÎncă nu există evaluări
- Nutrition: iGCSE BiologyDocument76 paginiNutrition: iGCSE Biologyviolet paul100% (1)
- Dáp An AvDocument32 paginiDáp An AvDũngNguyễnHữu100% (1)
- First Pillar of Integrative HealthDocument11 paginiFirst Pillar of Integrative HealthMus OubÎncă nu există evaluări
- Gastrointestinal System Disorders For PediaDocument92 paginiGastrointestinal System Disorders For PediaQuolette Constante100% (1)