S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- College of Physicians and Surgeons of Ontario's Affidavit Re: Eve's Laser ClinicDocument27 paginiCollege of Physicians and Surgeons of Ontario's Affidavit Re: Eve's Laser CliniccbcottawaÎncă nu există evaluări
- OC Transpo Winterlude Bus RoutesDocument1 paginăOC Transpo Winterlude Bus RoutescbcottawaÎncă nu există evaluări
- Statement From NCC Chair Russell Mills, Jan. 30, 2014Document2 paginiStatement From NCC Chair Russell Mills, Jan. 30, 2014cbcottawa100% (1)
- RCMP Officer Files Sexual Assault ClaimDocument42 paginiRCMP Officer Files Sexual Assault ClaimcbcottawaÎncă nu există evaluări
- Leighton Family Lawsuit Against School Board, TeacherDocument16 paginiLeighton Family Lawsuit Against School Board, TeachercbcottawaÎncă nu există evaluări
- Algonquin Land Claim Preliminary Draft AgreementDocument133 paginiAlgonquin Land Claim Preliminary Draft AgreementcbcottawaÎncă nu există evaluări
- 2012 Emerald Ash Borer MapDocument23 pagini2012 Emerald Ash Borer MapcbcottawaÎncă nu există evaluări
- MPS' Letter On LRTDocument2 paginiMPS' Letter On LRTDavidReevelyÎncă nu există evaluări
- Lansdowne Partnership PlanDocument18 paginiLansdowne Partnership PlancbcottawaÎncă nu există evaluări
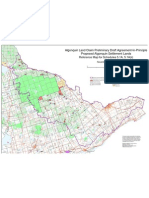
- Map of Proposed Algonquin Land Claim AgreementDocument1 paginăMap of Proposed Algonquin Land Claim Agreementcbcottawa50% (2)
- Constable Chris Getz Statement in Gregson TrialDocument3 paginiConstable Chris Getz Statement in Gregson TrialcbcottawaÎncă nu există evaluări
- Notice-Occupy Ottawa enDocument1 paginăNotice-Occupy Ottawa enTrevor PritchardÎncă nu există evaluări
- Factum of The RespondentDocument157 paginiFactum of The RespondentDavidReevelyÎncă nu există evaluări
- Friends of Lansdowne FactumDocument123 paginiFriends of Lansdowne Factumcbcottawa0% (1)
- Friends of Lansdowne and City of Ottawa Et AlDocument32 paginiFriends of Lansdowne and City of Ottawa Et AlDavidReevelyÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Application No.: 214/103698 Roll No.: EOG/CH/T/214/310Document3 paginiApplication No.: 214/103698 Roll No.: EOG/CH/T/214/310sathyajiÎncă nu există evaluări
- Punjab Armed Police Constables Jobs NotificationDocument9 paginiPunjab Armed Police Constables Jobs NotificationgovtjobsdailyÎncă nu există evaluări
- Managing Organizational CommunicationDocument9 paginiManaging Organizational CommunicationBeatriz VidalÎncă nu există evaluări
- An Analysis of Recruitment and Selection Process at UflexDocument37 paginiAn Analysis of Recruitment and Selection Process at Uflexanuojha123Încă nu există evaluări
- Job Interviews Tips and Techniques, Sample Interview Questions and AnswersDocument10 paginiJob Interviews Tips and Techniques, Sample Interview Questions and AnswersMohamed MokpelÎncă nu există evaluări
- WFOR-TV/WBFS-TV EEO Public File Report - 2021Document13 paginiWFOR-TV/WBFS-TV EEO Public File Report - 2021Alfred CharlesÎncă nu există evaluări
- Group6 GoogleDocument16 paginiGroup6 GoogleShivakshi SinghalÎncă nu există evaluări
- LinkedIn Emerging Jobs in The PhilippinesDocument24 paginiLinkedIn Emerging Jobs in The PhilippinesNoemi Lardizabal-Dado100% (1)
- Capr-Ii 6004Document54 paginiCapr-Ii 6004Sara PatilÎncă nu există evaluări
- Project Report On Navratann PVC Flex Banneremployees SatisfactionDocument49 paginiProject Report On Navratann PVC Flex Banneremployees SatisfactionHitesh Parmar100% (2)
- Talent Management Systems OverviewDocument3 paginiTalent Management Systems OverviewArpon DasÎncă nu există evaluări
- Maintenance Coordinator Cover LetterDocument6 paginiMaintenance Coordinator Cover Letterguj0zukyven2100% (2)
- Bank Exam Important PDFSDocument8 paginiBank Exam Important PDFSsecodarybksÎncă nu există evaluări
- Anatomy of A Great Cold Recruiting EmailDocument17 paginiAnatomy of A Great Cold Recruiting EmailAdaeze Princess NzekweÎncă nu există evaluări
- CC - Principles of - Management Chapter 5: Staffing Staffing Function of ManagementDocument15 paginiCC - Principles of - Management Chapter 5: Staffing Staffing Function of ManagementRahul DekaÎncă nu există evaluări
- HRM Practices in Infosys and TCSDocument10 paginiHRM Practices in Infosys and TCSshruthi mÎncă nu există evaluări
- Principles of Management - Travel CompanyDocument33 paginiPrinciples of Management - Travel CompanyChandra Sen BhatiaÎncă nu există evaluări
- Ultimate Guide To Writing A Perfect ResumeDocument18 paginiUltimate Guide To Writing A Perfect ResumeFrench frenzyÎncă nu există evaluări
- Chemical Engineering Career Pathways: SpecialisationsDocument6 paginiChemical Engineering Career Pathways: SpecialisationsfalyaÎncă nu există evaluări
- UnschoolDocument64 paginiUnschoolMUEKSH MANWANIÎncă nu există evaluări
- Online Recruitment Application (Ora) PreviewDocument6 paginiOnline Recruitment Application (Ora) Previewkamalshukla12Încă nu există evaluări
- 18th SCM New Points 1 JohxDocument55 pagini18th SCM New Points 1 JohxAnujit Shweta KulshresthaÎncă nu există evaluări
- Staffing in Organizations ASSIGNMENTDocument5 paginiStaffing in Organizations ASSIGNMENTManiÎncă nu există evaluări
- Home Depot ResumeDocument4 paginiHome Depot Resumenjoqvnjbf100% (2)
- Dessler Ch1Document31 paginiDessler Ch1amsÎncă nu există evaluări
- Sales Force Recruitment TrainingDocument27 paginiSales Force Recruitment TraininganashussainÎncă nu există evaluări
- HOMEWORK RH Selection and RecruitmentDocument4 paginiHOMEWORK RH Selection and RecruitmentThe Oumaima ElmaÎncă nu există evaluări
- SITXHRM004 Assessment 3 - ObservationsDocument12 paginiSITXHRM004 Assessment 3 - ObservationsRico SajaÎncă nu există evaluări
- HRM Short Course - Assignment - Jerry ModestoDocument2 paginiHRM Short Course - Assignment - Jerry ModestoJerry Ayagan ModestoÎncă nu există evaluări