S-ar putea să vă placă și
- A Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsDe la EverandA Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsÎncă nu există evaluări
- Extracapsular Cataract Extraction (ECCE) Is A Category of Eye Surgery in WhichDocument13 paginiExtracapsular Cataract Extraction (ECCE) Is A Category of Eye Surgery in WhichMa Christina RabayaÎncă nu există evaluări
- What Causes Cataract?Document3 paginiWhat Causes Cataract?Eye spacialistÎncă nu există evaluări
- Cataract: What You Should KnowDocument24 paginiCataract: What You Should KnowshinhyejjÎncă nu există evaluări
- Eye Disorders: Presented by Carmelita Ramos, RNDocument65 paginiEye Disorders: Presented by Carmelita Ramos, RNJayme_Galang_7078100% (1)
- PterygiumDocument3 paginiPterygiumtri_budi_20Încă nu există evaluări
- HemophiliaDocument4 paginiHemophiliaMechelle ChenÎncă nu există evaluări
- Retinal Vein Occlusion Concept MapDocument2 paginiRetinal Vein Occlusion Concept MapJoe RealÎncă nu există evaluări
- Eye Disorder in Childhood & Adolescent: Lia Meuthia Zaini FK Unsyiah / RSUZADocument54 paginiEye Disorder in Childhood & Adolescent: Lia Meuthia Zaini FK Unsyiah / RSUZACut MulianiÎncă nu există evaluări
- TrabeculectomyDocument28 paginiTrabeculectomyAlfu RafdiÎncă nu există evaluări
- CATARACTS and GLAUCOMADocument11 paginiCATARACTS and GLAUCOMAAmoroso, Marian Corneth D.Încă nu există evaluări
- Extracapsular Cataract Extraction (OR)Document4 paginiExtracapsular Cataract Extraction (OR)Jet-Jet GuillerganÎncă nu există evaluări
- Amyotrophic Lateral SclerosisDocument24 paginiAmyotrophic Lateral SclerosisJeanessa Delantar QuilisadioÎncă nu există evaluări
- Neuro-Ophta EditedDocument97 paginiNeuro-Ophta EditedMarshet GeteÎncă nu există evaluări
- Presented by Carmelita Ramos, RNDocument81 paginiPresented by Carmelita Ramos, RNMela De Jesus RamosÎncă nu există evaluări
- Reye's SyndromeDocument11 paginiReye's SyndromeChristine Go100% (1)
- Adults, Elderly and Children Over 1 YearDocument7 paginiAdults, Elderly and Children Over 1 YeardindaikaputriÎncă nu există evaluări
- Spina BifidaDocument6 paginiSpina BifidaAdiel Calsa100% (1)
- Guideline Surgical Wounds Primary Secondary Intention PDFDocument11 paginiGuideline Surgical Wounds Primary Secondary Intention PDFHanifwibowo MumtazÎncă nu există evaluări
- Study Guide 1 - Leadership and FollowershipDocument11 paginiStudy Guide 1 - Leadership and FollowershipMark Vincent GallenoÎncă nu există evaluări
- Wound Dressings Update: Carolina Weller, Geoff SussmanDocument7 paginiWound Dressings Update: Carolina Weller, Geoff SussmanyodinheimÎncă nu există evaluări
- Tibial FractureDocument6 paginiTibial FractureKristene June Ilagan CoyamÎncă nu există evaluări
- Spinal Cord Injury Case Study (Physical Assessment)Document3 paginiSpinal Cord Injury Case Study (Physical Assessment)TobiDaÎncă nu există evaluări
- 02 Preoperative Assessment of A Patient With Cataract-FinalDocument10 pagini02 Preoperative Assessment of A Patient With Cataract-Finalmdshahidalam315Încă nu există evaluări
- AnginaDocument17 paginiAnginaGaming ModeÎncă nu există evaluări
- Danger Signs of PregnancyDocument3 paginiDanger Signs of PregnancyNesly Khyrozz LorenzoÎncă nu există evaluări
- Intro-ESRD Case StudyDocument2 paginiIntro-ESRD Case StudyAngel SamonteÎncă nu există evaluări
- Asking Your Question (PICO) - NursingDocument5 paginiAsking Your Question (PICO) - NursingBentaigaÎncă nu există evaluări
- Clavicle Fractures Treatment & ManagementDocument11 paginiClavicle Fractures Treatment & ManagementshtefanazÎncă nu există evaluări
- NYCTALOPIADocument16 paginiNYCTALOPIAAroob YaseenÎncă nu există evaluări
- ENUCLEATIONDocument14 paginiENUCLEATIONBlessy SebastianÎncă nu există evaluări
- Ulcerative Colitis: DR Syed Ubaid Associate Professor of SurgeryDocument71 paginiUlcerative Colitis: DR Syed Ubaid Associate Professor of SurgeryFachry Al RafiqiÎncă nu există evaluări
- NR 283 Unit 1 DefinitionsDocument3 paginiNR 283 Unit 1 DefinitionsLeksis LoveÎncă nu există evaluări
- AstigmatismDocument1 paginăAstigmatismAmmellya PutriÎncă nu există evaluări
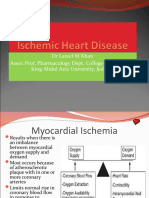
- Ischemic Heart Disease Revised LMKDocument50 paginiIschemic Heart Disease Revised LMKLateef KhanÎncă nu există evaluări
- Abcess CellulitisDocument60 paginiAbcess CellulitisKirk Kevin PolanteÎncă nu există evaluări
- Nursing Interview Guide To Collect Subjective Data From The Client Questions RationaleDocument19 paginiNursing Interview Guide To Collect Subjective Data From The Client Questions RationaleKent Rebong100% (1)
- Nursing Interventions in SchizophreniaDocument24 paginiNursing Interventions in SchizophreniaChristian Apelo Serquillos0% (1)
- Case Report No1Document9 paginiCase Report No1Menn PetchuayÎncă nu există evaluări
- Running Head: A Patient Who Has Glaucoma 1Document10 paginiRunning Head: A Patient Who Has Glaucoma 1Alonso LugoÎncă nu există evaluări
- Unstable AnginaDocument10 paginiUnstable AnginaironÎncă nu există evaluări
- Choking: by Jawad AhmedDocument25 paginiChoking: by Jawad Ahmedjawad_ahmedÎncă nu există evaluări
- Benign Prostate HyperplasiaDocument126 paginiBenign Prostate HyperplasiaJubaida JemiÎncă nu există evaluări
- 1 - Ocular TraumaDocument31 pagini1 - Ocular TraumadeoshiÎncă nu există evaluări
- 422 Shock EssayDocument6 pagini422 Shock Essayapi-364149810Încă nu există evaluări
- Head Injury Pamphlet PDFDocument2 paginiHead Injury Pamphlet PDFapi-279596675Încă nu există evaluări
- Physical Assessment External EyesDocument97 paginiPhysical Assessment External EyesDeeeeeÎncă nu există evaluări
- Toxic Megacolon Presentation FinalDocument33 paginiToxic Megacolon Presentation FinalHendra SetyawanÎncă nu există evaluări
- Cardiovascular Disease in The ElderlyDocument18 paginiCardiovascular Disease in The ElderlynfacmaÎncă nu există evaluări
- Reflection: Group 2 - Bojorque - Eupeña - Joya - Lastimosa - Martin - Quinto - SR - Robles - Sakay - Samillano - VilarDocument4 paginiReflection: Group 2 - Bojorque - Eupeña - Joya - Lastimosa - Martin - Quinto - SR - Robles - Sakay - Samillano - VilarMeccanazaren Susvilla BojorqueÎncă nu există evaluări
- Ward Case PresentationDocument92 paginiWard Case PresentationSuzette Rae TateÎncă nu există evaluări
- DIAGNOSTIC TEST Tonometry Corneal StainingDocument29 paginiDIAGNOSTIC TEST Tonometry Corneal StainingJhonelle ProdigalidadÎncă nu există evaluări
- A. Antineoplastic DrugsDocument48 paginiA. Antineoplastic DrugsKim Shyen BontuyanÎncă nu există evaluări
- Emergency Care - Near-DrowningDocument11 paginiEmergency Care - Near-DrowningdrileshkotechaÎncă nu există evaluări
- Preoperative Assessment in Diabetic PatientsDocument2 paginiPreoperative Assessment in Diabetic PatientsShilpa Pradhan100% (1)
- TendonitisDocument3 paginiTendonitisJingyi Xie0% (1)
- Narrative PathophysiologyDocument18 paginiNarrative PathophysiologyNica Georgelle Maniego SamonteÎncă nu există evaluări
- Ebook 20Document8 paginiEbook 20Eusivia PasiÎncă nu există evaluări
- Biology Invesigatory Project: Group MembersDocument13 paginiBiology Invesigatory Project: Group MembersNavaneeth KrishnanÎncă nu există evaluări
- Case Refraksi Lassa Anisometrop FinalDocument7 paginiCase Refraksi Lassa Anisometrop FinalRizkyAgustriaÎncă nu există evaluări
- Efek DM Pada MataDocument60 paginiEfek DM Pada MataRizkyAgustriaÎncă nu există evaluări
- Case Rekon JNDocument70 paginiCase Rekon JNRizkyAgustriaÎncă nu există evaluări
- Pseudo Aphakic GlaucomaDocument38 paginiPseudo Aphakic GlaucomaRizkyAgustriaÎncă nu există evaluări
- Phaco 11Document38 paginiPhaco 11RizkyAgustriaÎncă nu există evaluări
- Femtosecond Laser Cataract Surgery - Magic or Myth? A Balanced View!Document31 paginiFemtosecond Laser Cataract Surgery - Magic or Myth? A Balanced View!RizkyAgustriaÎncă nu există evaluări
- Phaco3 PDFDocument26 paginiPhaco3 PDFRizkyAgustriaÎncă nu există evaluări
- Choroidal Thickness in NAIONDocument7 paginiChoroidal Thickness in NAIONRizkyAgustriaÎncă nu există evaluări
- Weinstein SDocument4 paginiWeinstein SRizkyAgustriaÎncă nu există evaluări
- Phaco3 PDFDocument26 paginiPhaco3 PDFRizkyAgustriaÎncă nu există evaluări
- Entoptic PhenomenaDocument11 paginiEntoptic PhenomenaRizkyAgustriaÎncă nu există evaluări
- Phaco 11Document38 paginiPhaco 11RizkyAgustriaÎncă nu există evaluări
- Study Designs: Case-Control StudiesDocument119 paginiStudy Designs: Case-Control StudiesRizkyAgustriaÎncă nu există evaluări
- Frekuensi Crosstab AnovaDocument9 paginiFrekuensi Crosstab AnovaRizkyAgustriaÎncă nu există evaluări
- Urea 10Document3 paginiUrea 10RizkyAgustriaÎncă nu există evaluări
- Weinstein SDocument4 paginiWeinstein SRizkyAgustriaÎncă nu există evaluări
- Overview of Water and Environmental Sanitation in IndonesiaDocument1 paginăOverview of Water and Environmental Sanitation in IndonesiaRizkyAgustriaÎncă nu există evaluări
- Retinoblastoma: What Is Cancer?Document41 paginiRetinoblastoma: What Is Cancer?RizkyAgustriaÎncă nu există evaluări
- The Role of Systemic Treatments For Skin Lightening: Margit L. W. Juhasz MD MDDocument14 paginiThe Role of Systemic Treatments For Skin Lightening: Margit L. W. Juhasz MD MDDr. Bhawna GuptaÎncă nu există evaluări
- Spirulina CyanotechDocument22 paginiSpirulina CyanotechDineshhaa DineshÎncă nu există evaluări
- Trends in Food Science & Technology: Citrullus Lanatus As Source of Bioactive Components: An Up-To-Date ReviewDocument15 paginiTrends in Food Science & Technology: Citrullus Lanatus As Source of Bioactive Components: An Up-To-Date ReviewluciaÎncă nu există evaluări
- Chapter 17 - Nutritional Agents - 2008 - Clinical Ocular PharmacologyDocument7 paginiChapter 17 - Nutritional Agents - 2008 - Clinical Ocular PharmacologysÎncă nu există evaluări
- 0302 USNutra ViewDocument2 pagini0302 USNutra Viewpangsai3000Încă nu există evaluări
- Ajanta-Prisma Product DetailsDocument2 paginiAjanta-Prisma Product DetailsBalaji Pharmacy - GMÎncă nu există evaluări
- Lucovit EngDocument5 paginiLucovit EngstanionremusÎncă nu există evaluări
- Eagle Eyes by UniScience GroupDocument30 paginiEagle Eyes by UniScience GroupChen Wai PengÎncă nu există evaluări
- Effect of Light and Temperature On Stability of ZeaxanthinDocument19 paginiEffect of Light and Temperature On Stability of Zeaxanthinnoorain zulkapliÎncă nu există evaluări
- Power Foods For Daily Health and VitalityDocument38 paginiPower Foods For Daily Health and Vitalitycarpop52Încă nu există evaluări
- Functions, Therapeutic Applications, and Synthesis of Retinoids and CarotenoidsDocument125 paginiFunctions, Therapeutic Applications, and Synthesis of Retinoids and CarotenoidsJosué VelázquezÎncă nu există evaluări
- Regular Egg Consumption at Breakfast by Japanese Woman University Students Improves Daily Nutrient Intakes: Open-Labeled ObservationsDocument7 paginiRegular Egg Consumption at Breakfast by Japanese Woman University Students Improves Daily Nutrient Intakes: Open-Labeled ObservationsLeena MuniandyÎncă nu există evaluări
- Learn About CataractsDocument41 paginiLearn About CataractsRizkyAgustriaÎncă nu există evaluări
- LuteinDocument38 paginiLuteinirfanmuhfiÎncă nu există evaluări
- HarvestPlus Handbook For Carotenoid AnalysisDocument63 paginiHarvestPlus Handbook For Carotenoid AnalysisGuillermo MontoyaÎncă nu există evaluări
- Global Phytonutrient Report Commissioned by The Nutrilite Health InstituteDocument22 paginiGlobal Phytonutrient Report Commissioned by The Nutrilite Health Instituteโยอันนา ยุนอา แคทเธอรีน เอี่ยมสุวรรณÎncă nu există evaluări
- Artikel 1-Review Nutrasetikal Untuk LansiaDocument10 paginiArtikel 1-Review Nutrasetikal Untuk LansiaMade DesmantaÎncă nu există evaluări
- Rodriguez-Concepcion Et Al. - 2018 - Progress in Lipid Research A Global Perspective On Carotenoids Metabolism, Biotechnology, and Be-Annotated PDFDocument32 paginiRodriguez-Concepcion Et Al. - 2018 - Progress in Lipid Research A Global Perspective On Carotenoids Metabolism, Biotechnology, and Be-Annotated PDFEdna EdÎncă nu există evaluări
- Lutein and ZeaxanthinDocument17 paginiLutein and ZeaxanthinBabaÎncă nu există evaluări
- Increase in Lutein and Zeaxanthin Content in The Eggs PDFDocument8 paginiIncrease in Lutein and Zeaxanthin Content in The Eggs PDFAmit KumariÎncă nu există evaluări
- Carotenoids: Advances in Nutrition July 2013Document4 paginiCarotenoids: Advances in Nutrition July 2013Toàn MinhÎncă nu există evaluări
- Feeding For Designer EggsDocument14 paginiFeeding For Designer EggsDr. Vivek PatilÎncă nu există evaluări
- FloraGLO Specification SheetDocument2 paginiFloraGLO Specification SheetPaul Krawitz100% (1)
- Jus AlpukatDocument6 paginiJus Alpukatnurul istialiyahÎncă nu există evaluări
- Product Handbook: Aloe InspiredDocument56 paginiProduct Handbook: Aloe InspiredElegant Prince100% (1)
- USP Astec MarigoldDocument3 paginiUSP Astec MarigoldAnnastasia PiyogoÎncă nu există evaluări
- Biofortification Maize Storage - Taleon2017Document7 paginiBiofortification Maize Storage - Taleon2017Djibode EstherÎncă nu există evaluări
- Cookies ThesisDocument36 paginiCookies ThesisNegero Ararso100% (1)
- Eat by Color by DR David HeberDocument11 paginiEat by Color by DR David HeberCaraÎncă nu există evaluări
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (29)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (2)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe la EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsÎncă nu există evaluări
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe la EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionEvaluare: 4 din 5 stele4/5 (404)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (81)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe la EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsEvaluare: 3.5 din 5 stele3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDe la EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsEvaluare: 4.5 din 5 stele4.5/5 (170)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)De la EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Încă nu există evaluări
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 4 din 5 stele4/5 (6)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe la EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsEvaluare: 5 din 5 stele5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe la EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (42)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDe la EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessEvaluare: 4.5 din 5 stele4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDe la EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe la EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityEvaluare: 4 din 5 stele4/5 (5)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De la EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Evaluare: 4.5 din 5 stele4.5/5 (110)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisDe la EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisEvaluare: 5 din 5 stele5/5 (8)
- To Explain the World: The Discovery of Modern ScienceDe la EverandTo Explain the World: The Discovery of Modern ScienceEvaluare: 3.5 din 5 stele3.5/5 (51)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDe la EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisEvaluare: 3.5 din 5 stele3.5/5 (2)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Marshmallow Test: Mastering Self-ControlDe la EverandThe Marshmallow Test: Mastering Self-ControlEvaluare: 4.5 din 5 stele4.5/5 (59)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDe la EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryEvaluare: 4 din 5 stele4/5 (45)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDe la EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeEvaluare: 4.5 din 5 stele4.5/5 (253)