S-ar putea să vă placă și
- Nephrology NursingDocument1 paginăNephrology Nursingalexis_borjÎncă nu există evaluări
- Use of POCT To Help Inform Decision Making in Patients Over 65 Presenting With Acute Frailty SyndromeDocument17 paginiUse of POCT To Help Inform Decision Making in Patients Over 65 Presenting With Acute Frailty Syndromeنجلاء الطلحيÎncă nu există evaluări
- National Breast Cancer Audit Next StepsDocument14 paginiNational Breast Cancer Audit Next StepsumeshbhartiÎncă nu există evaluări
- Qsen Project Urinary Catheter ComplicationsDocument18 paginiQsen Project Urinary Catheter Complicationsapi-316643564Încă nu există evaluări
- PPP P: Jump To Indexing (Document Detils)Document6 paginiPPP P: Jump To Indexing (Document Detils)arriane_rosalesÎncă nu există evaluări
- Quality Assurance GuidelinesDocument28 paginiQuality Assurance Guidelinesmonir61Încă nu există evaluări
- 156 - A - Further Information RECIPEDocument6 pagini156 - A - Further Information RECIPEKeith userÎncă nu există evaluări
- C0876 - Advice On Maintaining Cancer Recovery - 30 November 2020Document5 paginiC0876 - Advice On Maintaining Cancer Recovery - 30 November 2020Kim Lee BrookÎncă nu există evaluări
- Chole - Protocol - V1-14, Birmingham, UK PDFDocument23 paginiChole - Protocol - V1-14, Birmingham, UK PDFWorku KifleÎncă nu există evaluări
- Does The Number of Operating Specialists Influence The Conversion Rate and Outcomes After Laparoscopic Colorectal Cancer Surgery?Document7 paginiDoes The Number of Operating Specialists Influence The Conversion Rate and Outcomes After Laparoscopic Colorectal Cancer Surgery?Yassine BahrÎncă nu există evaluări
- Best Practice Diagnostic Guidelines For Patients Presenting With Breast SymptomsDocument60 paginiBest Practice Diagnostic Guidelines For Patients Presenting With Breast SymptomsPratamasari Insani100% (2)
- Many Patients Will Experience Stool and Bowel Movement Related Symptoms After Treatment For Colorectal and Anal Cancer A Descriptive StudyDocument7 paginiMany Patients Will Experience Stool and Bowel Movement Related Symptoms After Treatment For Colorectal and Anal Cancer A Descriptive StudyAthenaeum Scientific PublishersÎncă nu există evaluări
- Gut 2011 Morris 806 13Document9 paginiGut 2011 Morris 806 13568563Încă nu există evaluări
- Rates of Anastomotic Complications and Their Management Following Esophagectomy - Results of The Oesophago-Gastric Anastomosis Audit (OGAA)Document44 paginiRates of Anastomotic Complications and Their Management Following Esophagectomy - Results of The Oesophago-Gastric Anastomosis Audit (OGAA)Агасиев МаликÎncă nu există evaluări
- Working Version - Palau Policy BriefDocument17 paginiWorking Version - Palau Policy BriefJoseph DreyÎncă nu există evaluări
- Research ArticleDocument8 paginiResearch Articleanon_44859125Încă nu există evaluări
- Nurse-Directed Interventions To Reduce Catheter-Associated Urinary Tract InfectionsDocument10 paginiNurse-Directed Interventions To Reduce Catheter-Associated Urinary Tract InfectionsAngernani Trias WulandariÎncă nu există evaluări
- 2012 Cancer System Quality Index - Erie St. Clair LHINDocument3 pagini2012 Cancer System Quality Index - Erie St. Clair LHINwindsorstarÎncă nu există evaluări
- Guide Lines in Surgical Quality ServiceDocument23 paginiGuide Lines in Surgical Quality ServiceAddis YeshitlaÎncă nu există evaluări
- The Effect of Integrating Early Palliative Care Modalities On Patients With Lung Cancer-1Document9 paginiThe Effect of Integrating Early Palliative Care Modalities On Patients With Lung Cancer-1api-396564080Încă nu există evaluări
- Atlas of Laparoscopic Gastrectomy for Gastric Cancer: High Resolution Image for New Surgical TechniqueDe la EverandAtlas of Laparoscopic Gastrectomy for Gastric Cancer: High Resolution Image for New Surgical TechniqueÎncă nu există evaluări
- Jurnal KadekDocument6 paginiJurnal KadekNikadek Ayu Dwi LestariÎncă nu există evaluări
- Saving Lives Averting CostsDocument79 paginiSaving Lives Averting CostsAbhishek DebÎncă nu există evaluări
- Care For Vulnerable Populations during COVID-19 Pandemic: Clinical Updates in COVID-19De la EverandCare For Vulnerable Populations during COVID-19 Pandemic: Clinical Updates in COVID-19Încă nu există evaluări
- 050 JCF Ent 0324 - JD & Ps EnglishDocument13 pagini050 JCF Ent 0324 - JD & Ps EnglishGhazalYaghoutdoustÎncă nu există evaluări
- Diagnosis Kanker Pankreas PDFDocument7 paginiDiagnosis Kanker Pankreas PDFAgustinus FatollaÎncă nu există evaluări
- Complicaciones y Costos de La Biopsia HepaticaDocument9 paginiComplicaciones y Costos de La Biopsia HepaticaYonatan Merchant PerezÎncă nu există evaluări
- Post-cholecystectomy Bile Duct InjuryDe la EverandPost-cholecystectomy Bile Duct InjuryVinay K. KapoorÎncă nu există evaluări
- 1 PBDocument3 pagini1 PBDessy Choerunnisa SuhermanÎncă nu există evaluări
- Anaesthesia For Pancreatic SurgeryDocument11 paginiAnaesthesia For Pancreatic SurgeryyenuginÎncă nu există evaluări
- Pathology Statement of IntentDocument10 paginiPathology Statement of IntentWilliams EkeneÎncă nu există evaluări
- Sign 87Document74 paginiSign 87Ng Wai SingÎncă nu există evaluări
- Management of Hepatocellular CarcinomaDocument21 paginiManagement of Hepatocellular CarcinomaOlgaÎncă nu există evaluări
- OC Guideline 2008Document8 paginiOC Guideline 2008Taufiqurrahman Abdul DjabbarÎncă nu există evaluări
- Top Trials in Gastroenterology & HepatologyDe la EverandTop Trials in Gastroenterology & HepatologyEvaluare: 4.5 din 5 stele4.5/5 (7)
- Principles of Oncology NursingDocument12 paginiPrinciples of Oncology NursingДария Коваленко100% (1)
- Endometriosis Care in Wales1Document81 paginiEndometriosis Care in Wales1Mary De la HozÎncă nu există evaluări
- Anesthesiaforemergency Abdominalsurgery: Carol Peden,, Michael J. ScottDocument13 paginiAnesthesiaforemergency Abdominalsurgery: Carol Peden,, Michael J. ScottJEFFERSON MUÑOZÎncă nu există evaluări
- Hospital Goal ExerciseDocument3 paginiHospital Goal ExercisedifferfromworldÎncă nu există evaluări
- Oncology NurseDocument4 paginiOncology NurseroesitaÎncă nu există evaluări
- Management of Peritoneal Metastases- Cytoreductive Surgery, HIPEC and BeyondDe la EverandManagement of Peritoneal Metastases- Cytoreductive Surgery, HIPEC and BeyondAditi BhattÎncă nu există evaluări
- Philippine Cancer Control Program.1.1Document8 paginiPhilippine Cancer Control Program.1.1Ruby Joy EspirituÎncă nu există evaluări
- Coursebook-Livertransplant ch27Document53 paginiCoursebook-Livertransplant ch27Сергей СадовниковÎncă nu există evaluări
- Saving Lives Averting CostsDocument79 paginiSaving Lives Averting CostsMedCR1987Încă nu există evaluări
- Perioperative Medicine: The Pathway To Better Surgical CareDocument28 paginiPerioperative Medicine: The Pathway To Better Surgical CareLee SungjongÎncă nu există evaluări
- Oncology NursingDocument6 paginiOncology NursingHonora Lisset Neri DionicioÎncă nu există evaluări
- Care For Vulnerable Populations During COVID-19 PandemicDe la EverandCare For Vulnerable Populations During COVID-19 PandemicÎncă nu există evaluări
- CPG Ulcer enDocument24 paginiCPG Ulcer enAlina BotnarencoÎncă nu există evaluări
- Jaime 12-12-16Document15 paginiJaime 12-12-16api-354204098Încă nu există evaluări
- Main 6Document8 paginiMain 6Nitin SharmaÎncă nu există evaluări
- DentistryDocument10 paginiDentistryAnonymous Cw1DGmRfÎncă nu există evaluări
- SG Website ExampleDocument21 paginiSG Website ExampleishwaryaÎncă nu există evaluări
- Articulo6 PDFDocument17 paginiArticulo6 PDFYerly Ramirez MuñozÎncă nu există evaluări
- Pi Is 0168827822030677Document10 paginiPi Is 0168827822030677Calin BurciuÎncă nu există evaluări
- Ade Et AlDocument7 paginiAde Et Alkang.asep008Încă nu există evaluări
- EBR - Cellular - Aberration - Fedelis, Cheryl Moana MarieDocument2 paginiEBR - Cellular - Aberration - Fedelis, Cheryl Moana MarieCheryl Moana Marie FedelisÎncă nu există evaluări
- Review of Acute Cancer Beds 1Document2 paginiReview of Acute Cancer Beds 1Cepi Ridwan FerdiansyahÎncă nu există evaluări
- 1 PDFDocument7 pagini1 PDFAndriawan BramÎncă nu există evaluări
- World Sepsis Day 2021 Webinar SlidesDocument74 paginiWorld Sepsis Day 2021 Webinar Slidessyukri alhamdaÎncă nu există evaluări
- Ompressions: Irway: Reathing:: Center For Professional Practice of Nursing CPR Guidelines For Health-Care ProvidersDocument11 paginiOmpressions: Irway: Reathing:: Center For Professional Practice of Nursing CPR Guidelines For Health-Care Providersmonir61Încă nu există evaluări
- 2016 CUSP A Framework For SuccessDocument31 pagini2016 CUSP A Framework For Successmonir61Încă nu există evaluări
- Coronary ThrombosisDocument1 paginăCoronary Thrombosismonir61Încă nu există evaluări
- Technique For Awake Fibre Optic IntubationDocument3 paginiTechnique For Awake Fibre Optic Intubationmonir61Încă nu există evaluări
- Update On PDPHDocument18 paginiUpdate On PDPHmonir61Încă nu există evaluări
- Calcium Homeostasis: Bone Blood Ca++ KidneyDocument12 paginiCalcium Homeostasis: Bone Blood Ca++ KidneyOmSilence2651Încă nu există evaluări
- PALS 2010 OverviewDocument26 paginiPALS 2010 Overviewmonir61Încă nu există evaluări
- TandA 9912Document50 paginiTandA 9912Vinod RajÎncă nu există evaluări
- Admission Nursing AssessmentDocument20 paginiAdmission Nursing Assessmentmonir61Încă nu există evaluări
- Improving The Patient Experience Through Nursing and Midwifery KpisDocument35 paginiImproving The Patient Experience Through Nursing and Midwifery Kpismonir61Încă nu există evaluări
- Brenda Creaney PresentationDocument21 paginiBrenda Creaney Presentationmonir61Încă nu există evaluări
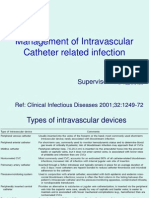
- Management of Intravascular Catheter Related InfectionDocument19 paginiManagement of Intravascular Catheter Related Infectionmonir61Încă nu există evaluări
- Tonsillectomy and AdiniodectomyDocument0 paginiTonsillectomy and Adiniodectomymonir61Încă nu există evaluări
- Hysterectomy: The American College of Obstetricians and GynecologistsDocument0 paginiHysterectomy: The American College of Obstetricians and Gynecologistsmonir61Încă nu există evaluări
- Cystoscopy: A Guide For WomenDocument2 paginiCystoscopy: A Guide For Womenmonir61Încă nu există evaluări
- LumbarlandDocument10 paginiLumbarlandmonir61Încă nu există evaluări
- ERCP-related Adverse Events: European Society of Gastrointestinal Endoscopy (ESGE) GuidelineDocument24 paginiERCP-related Adverse Events: European Society of Gastrointestinal Endoscopy (ESGE) GuidelineFarid RakhmanÎncă nu există evaluări
- Bile Duct StrictureDocument12 paginiBile Duct StricturechristianyecyecanÎncă nu există evaluări
- Imaging Spectrum of Duodenal EmergenciesDocument44 paginiImaging Spectrum of Duodenal EmergenciesJessi LaurentiusÎncă nu există evaluări
- Group 3 - Acute PancreatitisDocument5 paginiGroup 3 - Acute Pancreatitismelba040510Încă nu există evaluări
- Saint Louis University School of Medicine Mmxxii: Dr. Baldovino - October 13, 2020Document11 paginiSaint Louis University School of Medicine Mmxxii: Dr. Baldovino - October 13, 2020Djan Kurvie ValencerinaÎncă nu există evaluări
- Micro Tech Endoscopy Product CatalogDocument42 paginiMicro Tech Endoscopy Product CatalogyasuluÎncă nu există evaluări
- Tecnologías de Endoscopia - ECRIDocument5 paginiTecnologías de Endoscopia - ECRIJuliana cabrera corellaÎncă nu există evaluări
- Acute Cholangitis - An Overview of Management and TreatmentDocument9 paginiAcute Cholangitis - An Overview of Management and TreatmentJohn DoeÎncă nu există evaluări
- Management of Acute Pancreatitis - UpToDateDocument39 paginiManagement of Acute Pancreatitis - UpToDateYarlin MontoyaÎncă nu există evaluări
- Serology and Ultrasound For Diagnosis of Choledocolitiasis 2014Document5 paginiSerology and Ultrasound For Diagnosis of Choledocolitiasis 2014DannyÎncă nu există evaluări
- Update On The Management of Acute Pancreatitis.52Document7 paginiUpdate On The Management of Acute Pancreatitis.52Sebastian DeMarinoÎncă nu există evaluări
- Answers Surgery ExamDocument17 paginiAnswers Surgery ExamKing Bal94Încă nu există evaluări
- 2004 Emergency UltrasoundDocument226 pagini2004 Emergency Ultrasoundpgiaf5935100% (1)
- Acute PancreatitisDocument58 paginiAcute PancreatitissujithÎncă nu există evaluări
- Lecture 4 Biliary TreeDocument31 paginiLecture 4 Biliary TreeattooÎncă nu există evaluări
- Uw Health Job Description: Endoscopy Technician - LeadDocument2 paginiUw Health Job Description: Endoscopy Technician - LeadAnupam KumarÎncă nu există evaluări
- Clinical Manifestations, Diagnosis, and Staging of Exocrine Pancreatic Cancer - UpToDateDocument59 paginiClinical Manifestations, Diagnosis, and Staging of Exocrine Pancreatic Cancer - UpToDateVinicius VieiraÎncă nu există evaluări
- Pediatric Gastroenterology Fellowship Program Handbook 2017-2018Document37 paginiPediatric Gastroenterology Fellowship Program Handbook 2017-2018Ana-Mihaela BalanuțaÎncă nu există evaluări
- Final Grand Case-GeneralaoDocument110 paginiFinal Grand Case-GeneralaoLovely Hope LugatimanÎncă nu există evaluări
- PancreatitisDocument6 paginiPancreatitisMahaÎncă nu există evaluări
- Diseases of The PancreasDocument220 paginiDiseases of The PancreasStefan TrifuÎncă nu există evaluări
- Chronic Pancreatitis: PathophysiologyDocument7 paginiChronic Pancreatitis: PathophysiologyMadelaine De Arco J.Încă nu există evaluări
- 4 - Stenting For Benign and PDFDocument21 pagini4 - Stenting For Benign and PDFMahdi ShareghÎncă nu există evaluări
- Endoscopy: Accepted ManuscriptDocument37 paginiEndoscopy: Accepted ManuscriptShivaraj S AÎncă nu există evaluări
- Mrcs HepatobiliaryDocument40 paginiMrcs HepatobiliaryAdebisiÎncă nu există evaluări
- CHOLEDOCHOLITHIASISDocument38 paginiCHOLEDOCHOLITHIASISPrecious Cofreros100% (3)
- Surgery Paper 1 Viva QDocument46 paginiSurgery Paper 1 Viva QMusabbirÎncă nu există evaluări
- Acute Cholecystitis SMT IV 2021Document43 paginiAcute Cholecystitis SMT IV 2021Dandi PremaÎncă nu există evaluări
- LibraryDocument20 paginiLibraryospinu6780Încă nu există evaluări
- Neoplasias Cisticas Do PancreasDocument37 paginiNeoplasias Cisticas Do PancreasMoises BitencourtÎncă nu există evaluări