S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Din332 PDFDocument4 paginiDin332 PDFmateo100% (2)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Suture Chart EthiconDocument1 paginăSuture Chart EthiconelfangorssÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- 2011 Exam GeotechnicalDocument9 pagini2011 Exam GeotechnicalAhmed AwadallaÎncă nu există evaluări
- Thermo Scientific Belt Conveyor Scale HandbookDocument20 paginiThermo Scientific Belt Conveyor Scale HandbookEJECUTIVO_1Încă nu există evaluări
- Anatomy Relevant To CholecystectomyDocument7 paginiAnatomy Relevant To Cholecystectomyazuresea01Încă nu există evaluări
- A Novel Technique For Fundal Retraction of The Gallbladder in Single-Port CholecystectomyDocument5 paginiA Novel Technique For Fundal Retraction of The Gallbladder in Single-Port Cholecystectomyazuresea01Încă nu există evaluări
- Surgical SutureDocument1 paginăSurgical Sutureazuresea01Încă nu există evaluări
- Sweet's Syndrome Mimicking Alkali Burn - A Clinical ConundrumDocument3 paginiSweet's Syndrome Mimicking Alkali Burn - A Clinical Conundrumazuresea01Încă nu există evaluări
- Advances in Management of Thyroid CancerDocument49 paginiAdvances in Management of Thyroid Cancerazuresea01Încă nu există evaluări
- Laparoscopic Splenectomy-Evolution and Crrent StatusDocument8 paginiLaparoscopic Splenectomy-Evolution and Crrent Statusazuresea01Încă nu există evaluări
- Question and Ans.3Document153 paginiQuestion and Ans.3gangoorsgÎncă nu există evaluări
- Strain GuageDocument6 paginiStrain GuageChristian EspanolÎncă nu există evaluări
- Specifications: Comparison of Kajaria Tiles Parameters To International Standards Bib Iso-13006:2018-09Document1 paginăSpecifications: Comparison of Kajaria Tiles Parameters To International Standards Bib Iso-13006:2018-09omerÎncă nu există evaluări
- 2.basic Electrical Engineering PDFDocument152 pagini2.basic Electrical Engineering PDFkandavel71Încă nu există evaluări
- As 1012.11-2000 Methods of Testing Concrete - DeterminationDocument9 paginiAs 1012.11-2000 Methods of Testing Concrete - Determinationmm100% (1)
- 1.1 Waves and Particles According To Classical PhysicsDocument8 pagini1.1 Waves and Particles According To Classical PhysicsLUCKY KUSHWAHAÎncă nu există evaluări
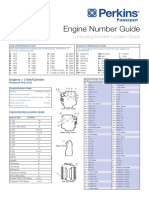
- Engine Number Guide (2-Page)Document2 paginiEngine Number Guide (2-Page)Abdul KhaliqÎncă nu există evaluări
- Quick Guide To Beam Analysis Using Strand7Document15 paginiQuick Guide To Beam Analysis Using Strand7Tarek AbulailÎncă nu există evaluări
- Observation Lesson in Physics DLP Activity 2 Now You Go Now Yu WontDocument2 paginiObservation Lesson in Physics DLP Activity 2 Now You Go Now Yu WontEmma Santua50% (2)
- Buting Senior High School Media and Information Literacy Unit TestDocument2 paginiButing Senior High School Media and Information Literacy Unit TestGina BundaÎncă nu există evaluări
- Error Analysis in Physics PDFDocument2 paginiError Analysis in Physics PDFKrystal0% (1)
- Wopho 13 Prob7-Final PDFDocument3 paginiWopho 13 Prob7-Final PDFPeter JonesÎncă nu există evaluări
- Shop Drawing Submittal: Project: Project No. Client: Consultant: Contractor: 20-373-DS-ARC-PE-21Document129 paginiShop Drawing Submittal: Project: Project No. Client: Consultant: Contractor: 20-373-DS-ARC-PE-21Ernest NavarroÎncă nu există evaluări
- Microplan - Katalog 2009 ENDocument18 paginiMicroplan - Katalog 2009 END.T.Încă nu există evaluări
- 2 SinteringDocument70 pagini2 SinteringMohammed Bilal100% (1)
- Ujian Nasional Bahasa Inggris SMA Tahun 1994Document6 paginiUjian Nasional Bahasa Inggris SMA Tahun 1994Andhika A. SetiyonoÎncă nu există evaluări
- HVAC Qualification KanishkDocument38 paginiHVAC Qualification Kanishkk.p.Încă nu există evaluări
- 117BP - CNC Technologies PDFDocument8 pagini117BP - CNC Technologies PDFvenkiscribd444Încă nu există evaluări
- C184 E037bDocument48 paginiC184 E037bNeyda Flores VasquezÎncă nu există evaluări
- Final Test: Grade: 3 Time: 30 Minutes Your Name: .. ScoreDocument8 paginiFinal Test: Grade: 3 Time: 30 Minutes Your Name: .. ScoreThu NguyenÎncă nu există evaluări
- F 1624 - 99 Rje2mjqtukveDocument8 paginiF 1624 - 99 Rje2mjqtukveJuanÎncă nu există evaluări
- Pipesim 2006.1 Fundamentals GasliftDocument13 paginiPipesim 2006.1 Fundamentals GasliftamulyanaÎncă nu există evaluări
- ESD in Fluid Lines: Theory and Application in The Petroleum and Aerospace IndustriesDocument5 paginiESD in Fluid Lines: Theory and Application in The Petroleum and Aerospace IndustriesKapil DevÎncă nu există evaluări
- Dr. Mukesh Kumar Department of Earthquake Engineering, NED University, KarachiDocument37 paginiDr. Mukesh Kumar Department of Earthquake Engineering, NED University, KarachiMukesh KumarÎncă nu există evaluări
- PEX250í 1200 Instruction ManualDocument10 paginiPEX250í 1200 Instruction ManualSebastian Aguila RaipanÎncă nu există evaluări
- Heat Pipe - Scientific AmericanDocument10 paginiHeat Pipe - Scientific AmericanEduardo Ocampo HernandezÎncă nu există evaluări
- Annual Plans 7th GradeDocument5 paginiAnnual Plans 7th GradeDiego Antonio RodriguezÎncă nu există evaluări