S-ar putea să vă placă și
- Everest 4x2 Titanium & Territory Titanium QuotationDocument2 paginiEverest 4x2 Titanium & Territory Titanium QuotationHerzl Hali V. HermosaÎncă nu există evaluări
- Cta Eb CV 01993 D 2020jun19 Ref PDFDocument20 paginiCta Eb CV 01993 D 2020jun19 Ref PDFHerzl Hali V. HermosaÎncă nu există evaluări
- Answer POEADocument6 paginiAnswer POEAHerzl Hali V. HermosaÎncă nu există evaluări
- RMC No. 102-2020 Annex ADocument2 paginiRMC No. 102-2020 Annex AHerzl Hali V. HermosaÎncă nu există evaluări
- Authorization Letter - BIRDocument1 paginăAuthorization Letter - BIRHerzl Hali V. Hermosa100% (1)
- Lay Me DownDocument2 paginiLay Me DownHerzl Hali V. HermosaÎncă nu există evaluări
- Establishment Report: Not For SaleDocument3 paginiEstablishment Report: Not For SaleHerzl Hali V. HermosaÎncă nu există evaluări
- Republic of The Philippines Quezon City: Court AppealsDocument38 paginiRepublic of The Philippines Quezon City: Court AppealsHerzl Hali V. HermosaÎncă nu există evaluări
- Aaron King Formal Offer 105Document3 paginiAaron King Formal Offer 105Herzl Hali V. HermosaÎncă nu există evaluări
- PCNCDocument4 paginiPCNCHerzl Hali V. HermosaÎncă nu există evaluări
- JuratDocument1 paginăJuratHerzl Hali V. HermosaÎncă nu există evaluări
- Conflict of LawsDocument3 paginiConflict of LawsHerzl Hali V. HermosaÎncă nu există evaluări
- Administrative Order No. Series of 2012: Republic of The Philippines Rtment of Social Welfare and DevelopmentDocument32 paginiAdministrative Order No. Series of 2012: Republic of The Philippines Rtment of Social Welfare and DevelopmentHerzl Hali V. HermosaÎncă nu există evaluări
- Industry OverviewDocument2 paginiIndustry OverviewHerzl Hali V. HermosaÎncă nu există evaluări
- ABRC2016.SCD2015.Remedial Law Revised Edited SegregateDocument8 paginiABRC2016.SCD2015.Remedial Law Revised Edited SegregateHerzl Hali V. HermosaÎncă nu există evaluări
- Review of Philippine Intellectual Property Law 1. TrademarksDocument5 paginiReview of Philippine Intellectual Property Law 1. TrademarksHerzl Hali V. HermosaÎncă nu există evaluări
- Special Power of AttorneyDocument1 paginăSpecial Power of AttorneyHerzl Hali V. HermosaÎncă nu există evaluări
- New Doc 2018-07-18 17.43.47 - 20180718174453 PDFDocument1 paginăNew Doc 2018-07-18 17.43.47 - 20180718174453 PDFHerzl Hali V. HermosaÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
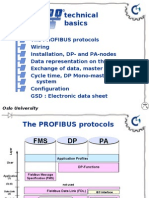
- Technical Basics: Oslo University CollegeDocument19 paginiTechnical Basics: Oslo University Collegesurendratv2007Încă nu există evaluări
- Math Olympiad Reviewer Grade 6Document7 paginiMath Olympiad Reviewer Grade 6Benz DyÎncă nu există evaluări
- S3 Ch7 Introduction To Probability QDocument17 paginiS3 Ch7 Introduction To Probability QF2D 10 FUNG SZE HANGÎncă nu există evaluări
- Mid Exam 2003Document17 paginiMid Exam 2003DavidÎncă nu există evaluări
- Image EnhancementDocument14 paginiImage EnhancementsanyamtimeÎncă nu există evaluări
- Modeling and Simulation of A Spray Column For NOx AbsorptionDocument15 paginiModeling and Simulation of A Spray Column For NOx AbsorptionAnel MamaniÎncă nu există evaluări
- Lab11 - Sequential System Design Using ASM ChartsDocument7 paginiLab11 - Sequential System Design Using ASM Chartswert1a2Încă nu există evaluări
- Workbook Full Solutions 2Document152 paginiWorkbook Full Solutions 2Muhammad MustafaÎncă nu există evaluări
- Mcqs For CSDDocument4 paginiMcqs For CSDBhautik DaxiniÎncă nu există evaluări
- Lecture22 3Document15 paginiLecture22 3Beverly PamanÎncă nu există evaluări
- High Speed Machining PresentationDocument36 paginiHigh Speed Machining Presentationsav33Încă nu există evaluări
- The Neural StrategyDocument102 paginiThe Neural StrategyGoran Stevanovic50% (2)
- Name: Charina Malolot-Villalon Exercise 4: Descriptive Statistics Instruction: Download Population Data at The Barangay Level of Your RespectiveDocument2 paginiName: Charina Malolot-Villalon Exercise 4: Descriptive Statistics Instruction: Download Population Data at The Barangay Level of Your RespectiveChrina MalolotÎncă nu există evaluări
- This Study Resource Was: Civil Engineering LawDocument3 paginiThis Study Resource Was: Civil Engineering LawCn cnÎncă nu există evaluări
- Project 11 - BJT and FET Amplifier Simulation and Analysis in ADS (February 2014)Document23 paginiProject 11 - BJT and FET Amplifier Simulation and Analysis in ADS (February 2014)Stephen J. Watt100% (2)
- Ged 102 Exercise 3 Module 1 1Q 2021-2022Document3 paginiGed 102 Exercise 3 Module 1 1Q 2021-2022DES MOSÎncă nu există evaluări
- Electric Field and Potential Lab ReportDocument6 paginiElectric Field and Potential Lab ReportAudio books LibraryÎncă nu există evaluări
- NT All PPRDocument20 paginiNT All PPRNagraj RaningaÎncă nu există evaluări
- Johannes Diderik Van Der WaalsDocument8 paginiJohannes Diderik Van Der WaalsPhilonious PhunkÎncă nu există evaluări
- Chuckra 11+ Maths Test 1Document9 paginiChuckra 11+ Maths Test 1ayesha safdarÎncă nu există evaluări
- Calculation of The Equivalent Resistance and Impedance of The Cylindrical Network Based On Recursion-Transform MethodDocument12 paginiCalculation of The Equivalent Resistance and Impedance of The Cylindrical Network Based On Recursion-Transform Methodmark_990566444Încă nu există evaluări
- 07 Solutions RegressionDocument74 pagini07 Solutions Regressionijaz afzal50% (2)
- Lesson Plan NBA-Operations ResearchDocument19 paginiLesson Plan NBA-Operations ResearchsunilmeÎncă nu există evaluări
- SME3013 History of Mathematical Sciences: SEMESTER 1 SESSION 2019/2020Document2 paginiSME3013 History of Mathematical Sciences: SEMESTER 1 SESSION 2019/2020Nur Hana SyamsulÎncă nu există evaluări
- 02 Chapter 2Document28 pagini02 Chapter 2ahmmed alhadad123Încă nu există evaluări
- Km31401 Makmal IV AcDocument3 paginiKm31401 Makmal IV AcChee OnnÎncă nu există evaluări
- Matrix Computation For Engineers and Scientist by JenningsDocument348 paginiMatrix Computation For Engineers and Scientist by JenningsAnonymous LcR6ykPBTÎncă nu există evaluări
- Sanskrit Sample Paper For PHD at IIT BDocument2 paginiSanskrit Sample Paper For PHD at IIT BShashankÎncă nu există evaluări
- Topic 3 Tape CorrectionsDocument38 paginiTopic 3 Tape CorrectionsShaine GaleraÎncă nu există evaluări
- Week 4 DLL-WK-13-LC-2021Document15 paginiWeek 4 DLL-WK-13-LC-2021Jerson YhuwelÎncă nu există evaluări