S-ar putea să vă placă și
- 3 12 13 BakrisDocument39 pagini3 12 13 BakrisJuliana FeronÎncă nu există evaluări
- Jurnal Gayon NosariaDocument16 paginiJurnal Gayon Nosariali mei fenÎncă nu există evaluări
- Click The Link and Go To Link - Running Man Ep 145 Eng Sub Is Up 6Document46 paginiClick The Link and Go To Link - Running Man Ep 145 Eng Sub Is Up 6li mei fenÎncă nu există evaluări
- A Retrospective Analysis of Adenoidal Size in Children With Allergic Rhinitis and Nonallergic Idiopathic RhinitisDocument5 paginiA Retrospective Analysis of Adenoidal Size in Children With Allergic Rhinitis and Nonallergic Idiopathic Rhinitisli mei fenÎncă nu există evaluări
- CellulitisDocument17 paginiCellulitisli mei fenÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Esaote MyLab40 BrochureDocument8 paginiEsaote MyLab40 BrochureDiegoÎncă nu există evaluări
- Faktor Determinan Psikososial Dan Mediko Obstetrik Pada Pasien InggrisDocument15 paginiFaktor Determinan Psikososial Dan Mediko Obstetrik Pada Pasien Inggrisandika setionoÎncă nu există evaluări
- Case Study TulsiDocument13 paginiCase Study TulsiPranay ChaturvediÎncă nu există evaluări
- Cad Effectiveness of Smartphone-Based Mindfulness Training On Maternal Perinatal Depression Randomized Controlled TrialDocument23 paginiCad Effectiveness of Smartphone-Based Mindfulness Training On Maternal Perinatal Depression Randomized Controlled TrialZir LakedÎncă nu există evaluări
- Flyer SugiesDocument2 paginiFlyer SugiesInomy ClaudiaÎncă nu există evaluări
- Registered Nurse ER Job Description in AustraliaDocument7 paginiRegistered Nurse ER Job Description in AustraliaAlex PiecesÎncă nu există evaluări
- FAST ExamDocument123 paginiFAST ExamSinisa Ristic50% (2)
- Congenital Pseudoarthrosis of The Clavicle A Rare CaseDocument5 paginiCongenital Pseudoarthrosis of The Clavicle A Rare CaseInternational Medical PublisherÎncă nu există evaluări
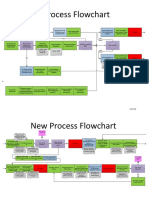
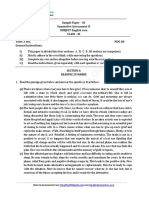
- New Process Flowchart CPOEDocument4 paginiNew Process Flowchart CPOELiza GeorgeÎncă nu există evaluări
- Free Paper Abstract BookDocument1.047 paginiFree Paper Abstract Bookkukadiya100% (1)
- Daftar Peralatan Elektromedik Menurut Ecri Dan WhoDocument4 paginiDaftar Peralatan Elektromedik Menurut Ecri Dan WhoAulia ArthaÎncă nu există evaluări
- A Whole New Ball GameDocument3 paginiA Whole New Ball GameFootball Club AllianzÎncă nu există evaluări
- Baruim SwallowDocument3 paginiBaruim SwallowCafferina VibranceliÎncă nu există evaluări
- Pebc TextbooksDocument3 paginiPebc TextbooksJhun0% (1)
- Congenital Anophthalmos in Benin CityDocument3 paginiCongenital Anophthalmos in Benin CityLjubomirErdoglijaÎncă nu există evaluări
- GENERAL HOSPITAL DESIGN SSTDocument19 paginiGENERAL HOSPITAL DESIGN SSTmamona zaheerÎncă nu există evaluări
- (B-0270) Day Surgery Procedure UnitDocument22 pagini(B-0270) Day Surgery Procedure UnitAhmad Gamal Elden MAhanyÎncă nu există evaluări
- Diagnostic Radiology Lab Part 2 Answer SheetDocument8 paginiDiagnostic Radiology Lab Part 2 Answer SheetVictoria Sosa100% (1)
- Franz Anton Mesmer His Life and Teaching by INCEDocument62 paginiFranz Anton Mesmer His Life and Teaching by INCEDidactylos1Încă nu există evaluări
- E A R D o C 2010 InvDocument16 paginiE A R D o C 2010 InvBarak ShitritÎncă nu există evaluări
- Pos&Ane&Car&Sym&Dia&Man&Hei&1 STDocument387 paginiPos&Ane&Car&Sym&Dia&Man&Hei&1 STJorge Luis VanegasÎncă nu există evaluări
- Infant Cranial UltrasoundDocument73 paginiInfant Cranial Ultrasoundg1381821100% (1)
- Male Internal Genital OrganDocument10 paginiMale Internal Genital OrganfiansisÎncă nu există evaluări
- In-Service Training Programs For Nurses, 1st and 2nd Quarter, Calendar Year 2023Document4 paginiIn-Service Training Programs For Nurses, 1st and 2nd Quarter, Calendar Year 2023iamxai rnmanemtÎncă nu există evaluări
- Caculba P2wk1-Gosodpa-Rle Day 2Document4 paginiCaculba P2wk1-Gosodpa-Rle Day 2Joyce Mae Vega SarmientoÎncă nu există evaluări
- Roman Catholic: Lucena City, PHDocument4 paginiRoman Catholic: Lucena City, PHJennet RiveraÎncă nu există evaluări
- Biometry by Suryakant Jha and Wangchuk Doma PDFDocument5 paginiBiometry by Suryakant Jha and Wangchuk Doma PDFJavier Andrés Pinochet SantoroÎncă nu există evaluări
- Morton's Metatarsalgia - Pathogenesis, Aetiology and Current ManagementDocument10 paginiMorton's Metatarsalgia - Pathogenesis, Aetiology and Current ManagementLikhit NayakÎncă nu există evaluări
- Case Pres ZandiOrstDocument17 paginiCase Pres ZandiOrstNajeeb UllahÎncă nu există evaluări
- Sample Paper 3Document8 paginiSample Paper 3Aswajith K BabuÎncă nu există evaluări