S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Evidence Kit: The Labyrinth: Remnants, Hints, and Desperate ObfuscationsDocument56 paginiEvidence Kit: The Labyrinth: Remnants, Hints, and Desperate ObfuscationsJoseph Robinson67% (9)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Fantasy - Portal Realms - 4EDocument35 paginiFantasy - Portal Realms - 4EAkmun Ra100% (4)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Cyberpunk Book ListDocument2 paginiCyberpunk Book ListJoseph RobinsonÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Endocrine CreditDocument58 paginiEndocrine CreditGiridhar SolasaÎncă nu există evaluări
- List of Space Marine ChaptersDocument55 paginiList of Space Marine ChaptersJoseph RobinsonÎncă nu există evaluări
- List of Space Marine ChaptersDocument55 paginiList of Space Marine ChaptersJoseph RobinsonÎncă nu există evaluări
- Hyperthyroidism 2011Document30 paginiHyperthyroidism 2011Elyza MagsaysayÎncă nu există evaluări
- Pretest EndocrineDocument2 paginiPretest EndocrineYuxin LiuÎncă nu există evaluări
- Clinical Endocrinology of Dogs Cats PDFDocument353 paginiClinical Endocrinology of Dogs Cats PDFsanjagruborovicÎncă nu există evaluări
- Codex Grots 8th Ed Home BrewDocument22 paginiCodex Grots 8th Ed Home BrewJoseph RobinsonÎncă nu există evaluări
- Congenital HypothyroidismDocument2 paginiCongenital Hypothyroidismapi-321672273Încă nu există evaluări
- Endocrine NCLEX PN Pract & ANS Questions IIDocument13 paginiEndocrine NCLEX PN Pract & ANS Questions IIYA HOÎncă nu există evaluări
- 101 Starship Cargos: SOS - Space Opera SupportDocument1 pagină101 Starship Cargos: SOS - Space Opera SupportJoseph RobinsonÎncă nu există evaluări
- CAJMTC MIM ED002.8 42x66Document1 paginăCAJMTC MIM ED002.8 42x66Joseph RobinsonÎncă nu există evaluări
- The Jugger Arizona Rulebook 2019-2020Document10 paginiThe Jugger Arizona Rulebook 2019-2020Joseph RobinsonÎncă nu există evaluări
- 75 State Street, 22nd Floor Boston, MA 02109 4707 Executive Drive San Diego, CA 92121 1055 LPL Way Fort Mill, SC 29715Document2 pagini75 State Street, 22nd Floor Boston, MA 02109 4707 Executive Drive San Diego, CA 92121 1055 LPL Way Fort Mill, SC 29715Joseph RobinsonÎncă nu există evaluări
- Au 2020 AJL Rulebook 51Document34 paginiAu 2020 AJL Rulebook 51Joseph RobinsonÎncă nu există evaluări
- Drills With ScottDocument2 paginiDrills With ScottJoseph RobinsonÎncă nu există evaluări
- The Lord Militant Giveth No FucksDocument1 paginăThe Lord Militant Giveth No FucksJoseph RobinsonÎncă nu există evaluări
- Puppets of Mirth Race of ConstuctsDocument39 paginiPuppets of Mirth Race of ConstuctsJoseph RobinsonÎncă nu există evaluări
- Kill Team Crawler v02Document11 paginiKill Team Crawler v02Joseph RobinsonÎncă nu există evaluări
- 25 Reasons Aliens Should Be Afraid of HumansDocument2 pagini25 Reasons Aliens Should Be Afraid of HumansJoseph RobinsonÎncă nu există evaluări
- 8th Ed Mission Draft V1.11Document16 pagini8th Ed Mission Draft V1.11Joseph RobinsonÎncă nu există evaluări
- 20,000 Nazis surrender to 83rd Infantry DivisionDocument4 pagini20,000 Nazis surrender to 83rd Infantry DivisionJoseph RobinsonÎncă nu există evaluări
- The Lord Militant Giveth No FucksDocument1 paginăThe Lord Militant Giveth No FucksJoseph RobinsonÎncă nu există evaluări
- Annual Training 15 Scenario: BN HQDocument2 paginiAnnual Training 15 Scenario: BN HQJoseph RobinsonÎncă nu există evaluări
- Potatoe Head StompaDocument67 paginiPotatoe Head StompaJoseph RobinsonÎncă nu există evaluări
- Potatoe Head StompaDocument67 paginiPotatoe Head StompaJoseph RobinsonÎncă nu există evaluări
- 2014 Best Warrior Competition AARDocument1 pagină2014 Best Warrior Competition AARJoseph RobinsonÎncă nu există evaluări
- 20,000 Nazis surrender to 83rd Infantry DivisionDocument4 pagini20,000 Nazis surrender to 83rd Infantry DivisionJoseph RobinsonÎncă nu există evaluări
- City Aflame PDFDocument1 paginăCity Aflame PDFJoseph RobinsonÎncă nu există evaluări
- City Aflame PDFDocument1 paginăCity Aflame PDFJoseph RobinsonÎncă nu există evaluări
- Annual Training Time Line Ideas 2015Document2 paginiAnnual Training Time Line Ideas 2015Joseph RobinsonÎncă nu există evaluări
- 40 K Narrative To MeDocument54 pagini40 K Narrative To MeJoseph RobinsonÎncă nu există evaluări
- Targeting Ideas For atDocument2 paginiTargeting Ideas For atJoseph RobinsonÎncă nu există evaluări
- Headhunter AwardDocument3 paginiHeadhunter AwardJoseph RobinsonÎncă nu există evaluări
- Austin Journal of Nephrology and HypertensionDocument4 paginiAustin Journal of Nephrology and HypertensionAustin Publishing GroupÎncă nu există evaluări
- Exam 1 PracticumDocument9 paginiExam 1 Practicumapi-310181843Încă nu există evaluări
- Kajian Patofisiologis Gejala Klinis dan Psikososial pada Wanita UsiDocument14 paginiKajian Patofisiologis Gejala Klinis dan Psikososial pada Wanita UsiSintia VeronikaÎncă nu există evaluări
- Endocrinologcazuri LP Limba EnglezăDocument17 paginiEndocrinologcazuri LP Limba EnglezăAna AlexandraÎncă nu există evaluări
- Individual Assigment IDDDocument3 paginiIndividual Assigment IDDSamsung A30sÎncă nu există evaluări
- PROPYLTHIOURACILDocument35 paginiPROPYLTHIOURACILMagdy Ali ELsherbenyÎncă nu există evaluări
- Thyroid Hormone Profile in Chronic Kidney DiseaseDocument6 paginiThyroid Hormone Profile in Chronic Kidney DiseaserefaÎncă nu există evaluări
- Hypothyroidism Case FileDocument2 paginiHypothyroidism Case Filehttps://medical-phd.blogspot.comÎncă nu există evaluări
- THYROID YunitaDocument81 paginiTHYROID YunitaPandu KusumawardhanyÎncă nu există evaluări
- Category Code and Author ListingDocument33 paginiCategory Code and Author Listingpriya selvarajÎncă nu există evaluări
- Thyroid Gland: Pactical Activity No. 5Document19 paginiThyroid Gland: Pactical Activity No. 5Damian CorinaÎncă nu există evaluări
- Pre Exam Surgical Notes 2Document166 paginiPre Exam Surgical Notes 2flor vickyÎncă nu există evaluări
- Hyperthyroidism & HypothyroidismDocument6 paginiHyperthyroidism & HypothyroidismRishikaphriya RauichandranÎncă nu există evaluări
- Nursing Management of Endocrine DisordersDocument7 paginiNursing Management of Endocrine Disorderslpirman05Încă nu există evaluări
- Diagnosing and managing pituitary and hypothalamic disordersDocument111 paginiDiagnosing and managing pituitary and hypothalamic disordersLiav KfirÎncă nu există evaluări
- Myxedema ComaDocument14 paginiMyxedema Comabc3bhat6206Încă nu există evaluări
- Benign Diseases of ThyroidDocument70 paginiBenign Diseases of ThyroidMounica MekalaÎncă nu există evaluări
- Medical Management of Children With Down SyndromeDocument8 paginiMedical Management of Children With Down SyndromeMariana OrozcoÎncă nu există evaluări
- Amiodarone & Thyroid Disease JCEM 2010Document8 paginiAmiodarone & Thyroid Disease JCEM 2010IffatNaeemÎncă nu există evaluări
- HHS Public Access: HypothyroidismDocument27 paginiHHS Public Access: HypothyroidismBrama AtmajaÎncă nu există evaluări
- The Nutritional Relationships of Vitamin A PDFDocument4 paginiThe Nutritional Relationships of Vitamin A PDFNikhilÎncă nu există evaluări
- BSN Oliveros, Leoneil B. Reading HypothyroidismDocument7 paginiBSN Oliveros, Leoneil B. Reading HypothyroidismleoÎncă nu există evaluări
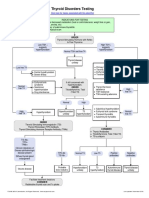
- Thyroid Testing AlgorithmDocument1 paginăThyroid Testing AlgorithmRezi HelperÎncă nu există evaluări
- 03.cleveland Clinic of Pediatrics - Selected Questions PDFDocument17 pagini03.cleveland Clinic of Pediatrics - Selected Questions PDFLakshaya SinghÎncă nu există evaluări