S-ar putea să vă placă și
- Exercices 41 CorrigeDocument11 paginiExercices 41 Corrige130660LYC OMAR BENABDELAZIZ NEDROMAÎncă nu există evaluări
- Catalogo de Despiece Cx290bDocument758 paginiCatalogo de Despiece Cx290bJoseph Romero100% (1)
- Chapitre IV La Formation ContinueDocument9 paginiChapitre IV La Formation ContinueAbdellah Moulay AlaouiÎncă nu există evaluări
- Cross-Culturel ConsDocument25 paginiCross-Culturel ConsMajid MezziÎncă nu există evaluări
- Etat Cond BQ Bna 2017Document5 paginiEtat Cond BQ Bna 2017Mouhamed SedkiÎncă nu există evaluări
- GENERALITES Et Introduction AnatomieDocument51 paginiGENERALITES Et Introduction AnatomieAbdellah Toubal SeghirÎncă nu există evaluări
- Jean-Pierre Vallarino - Les 10 Meilleurs Tours de Cartes AutomatiquesDocument1 paginăJean-Pierre Vallarino - Les 10 Meilleurs Tours de Cartes AutomatiquesAlex ButlovÎncă nu există evaluări
- DSP A 0115gqvDocument10 paginiDSP A 0115gqvMarc DutreuilÎncă nu există evaluări
- Reprise en Sous Sol Dcn5Document7 paginiReprise en Sous Sol Dcn5Far FarhaanÎncă nu există evaluări
- 1449159285Document17 pagini1449159285bensofienÎncă nu există evaluări
- Interet SimpleDocument21 paginiInteret SimpleLacenÎncă nu există evaluări
- La Géométrie Des SurfacesDocument3 paginiLa Géométrie Des Surfacesabd erahimÎncă nu există evaluări
- Livres Sur Estimation Appartement Le Bourget Vous Devriez LireDocument4 paginiLivres Sur Estimation Appartement Le Bourget Vous Devriez LiremachilohfwÎncă nu există evaluări
- Amortissement CoursDocument14 paginiAmortissement CoursponomarevaoÎncă nu există evaluări
- Clavette Et CirclipsDocument4 paginiClavette Et CirclipsMécanique 2019Încă nu există evaluări
- IT 246 - DésenfumageDocument12 paginiIT 246 - DésenfumageBenoit BARREREÎncă nu există evaluări
- 0089492-OMCompr-fr GEA Grasso Pistons PDFDocument18 pagini0089492-OMCompr-fr GEA Grasso Pistons PDFChristian CotteÎncă nu există evaluări
- Annexe 3 - 2018 FRDocument234 paginiAnnexe 3 - 2018 FRAli Ali100% (1)
- Bor 2013Document3 paginiBor 2013Mounia BELAIDÎncă nu există evaluări
- Grossesses À RisqueDocument3 paginiGrossesses À RisqueAsma TurkiÎncă nu există evaluări
- Programmation Annuelle 2023 Sciences Et TechnologiesDocument3 paginiProgrammation Annuelle 2023 Sciences Et TechnologieskittynoumeaÎncă nu există evaluări
- C3-INS PA 02 Conservation Des Echantillons BiologiquesDocument15 paginiC3-INS PA 02 Conservation Des Echantillons BiologiquesFaiza BouchalaÎncă nu există evaluări
- CM1 Introduction Systemes DistribuesDocument12 paginiCM1 Introduction Systemes DistribuesCharlotte SimoÎncă nu există evaluări
- Fiche Outil EleveDocument6 paginiFiche Outil ElevejosephÎncă nu există evaluări
- Gestion Administratif Du PersonnelDocument11 paginiGestion Administratif Du Personnellesyeuxdamla100% (1)
- Correction Des Exercices Du Chapitre 7: Exercice N° 12 P 143Document2 paginiCorrection Des Exercices Du Chapitre 7: Exercice N° 12 P 143aaraycheÎncă nu există evaluări
- Voix PassiveDocument4 paginiVoix PassiveHabibÎncă nu există evaluări
- Win Timdouine 2012 - Jean IsbecqueDocument15 paginiWin Timdouine 2012 - Jean IsbecquelluisaurouxÎncă nu există evaluări
- Diffusion Élastique Et Inélastique Des ProtonsDocument47 paginiDiffusion Élastique Et Inélastique Des Protonscharaf lÎncă nu există evaluări
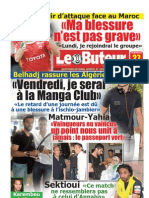
- LE BUTEUR PDF Du 27/05/2011Document24 paginiLE BUTEUR PDF Du 27/05/2011PDF JournalÎncă nu există evaluări