S-ar putea să vă placă și
- Imaging Techniques in Glaucoma: Presenter: Dr. Rujuta Moderator: Dr. Rita DhamankarDocument54 paginiImaging Techniques in Glaucoma: Presenter: Dr. Rujuta Moderator: Dr. Rita Dhamankardrvishalkulkarni2007Încă nu există evaluări
- RCollOph Guidelines For DRDocument14 paginiRCollOph Guidelines For DRdrvishalkulkarni2007Încă nu există evaluări
- Diabetic Macular EdemaDocument23 paginiDiabetic Macular Edemadrvishalkulkarni2007Încă nu există evaluări
- Showphacomrphic Glaucoma Managemnet by Surgical and Medical Management TextDocument8 paginiShowphacomrphic Glaucoma Managemnet by Surgical and Medical Management Textdrvishalkulkarni2007Încă nu există evaluări
- Amelanotic Melanoma.............................Document1 paginăAmelanotic Melanoma.............................drvishalkulkarni2007Încă nu există evaluări
- Penetrating Keratoplasty in Active Acanthamoeba KeratitisDocument5 paginiPenetrating Keratoplasty in Active Acanthamoeba Keratitisdrvishalkulkarni2007Încă nu există evaluări
- 001 PDFDocument2 pagini001 PDFdrvishalkulkarni2007Încă nu există evaluări
- Characteristics and Surgical Outcomes of Paediatric Retinal DetachmentDocument4 paginiCharacteristics and Surgical Outcomes of Paediatric Retinal Detachmentdrvishalkulkarni2007Încă nu există evaluări
- Intra OcularTumoursDocument35 paginiIntra OcularTumoursdrvishalkulkarni2007100% (1)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- NCP Blurred VisionDocument3 paginiNCP Blurred Visionناديه المعمريÎncă nu există evaluări
- Un M¿ Vsa Ssãv 2008 P/PHCN Ahkm/Xobxn 7.11.2007Document16 paginiUn M¿ Vsa Ssãv 2008 P/PHCN Ahkm/Xobxn 7.11.2007Shine PrabhakaranÎncă nu există evaluări
- 8 Science 16 Light TextBook QnADocument20 pagini8 Science 16 Light TextBook QnAkumaran RÎncă nu există evaluări
- Final Project DocumentationDocument7 paginiFinal Project Documentationradu danielÎncă nu există evaluări
- Ophthalmic Diseases and Their Homoeopathic Therapeutics A B Norton.01216 - 1Document15 paginiOphthalmic Diseases and Their Homoeopathic Therapeutics A B Norton.01216 - 1Jhakhar WelfareSocietyÎncă nu există evaluări
- Previous Paper NEET AIIMS Q - 1 To 97Document13 paginiPrevious Paper NEET AIIMS Q - 1 To 97Rahul UÎncă nu există evaluări
- Abnormal Pupil, How To DoDocument8 paginiAbnormal Pupil, How To DoUNHAS OphthalmologyÎncă nu există evaluări
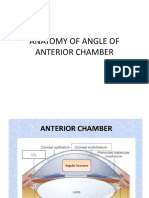
- Anatomy of Angle of Anterior ChamberDocument67 paginiAnatomy of Angle of Anterior ChamberRahnaÎncă nu există evaluări
- Gambaran Penderita Infeksi Mata Di Rumah Sakit Mata Manado Provinsi Sulawesi Utara Periode Juni 2017 - Juni 2019Document5 paginiGambaran Penderita Infeksi Mata Di Rumah Sakit Mata Manado Provinsi Sulawesi Utara Periode Juni 2017 - Juni 2019Darwin ThenÎncă nu există evaluări
- Attitude V6 Model Fsv1124 User Manual: Fat Shark 1Document12 paginiAttitude V6 Model Fsv1124 User Manual: Fat Shark 1Ronaldo PassanhaÎncă nu există evaluări
- Coding Poli Mata: Papillitis H46 Hypertension Ocular:h40.0 Macula H35.8 Ptosis H02.4 Chalazion H00.1 Asthenopia H53.1Document1 paginăCoding Poli Mata: Papillitis H46 Hypertension Ocular:h40.0 Macula H35.8 Ptosis H02.4 Chalazion H00.1 Asthenopia H53.1nurcasanÎncă nu există evaluări
- Retinoscopie 1 PDFDocument33 paginiRetinoscopie 1 PDFDiana LupoiuÎncă nu există evaluări
- Vision Development - Newborn To 12 Months - American Academy of OphthalmologyDocument2 paginiVision Development - Newborn To 12 Months - American Academy of Ophthalmologysneha duttaÎncă nu există evaluări
- Eye Fixation For HistologyDocument15 paginiEye Fixation For HistologyAlison AbreuÎncă nu există evaluări
- Specifications: Operating Instructions: Just Press StartDocument2 paginiSpecifications: Operating Instructions: Just Press StartHAITHM MURSHED0% (1)
- Veterinary Ophthalmic Surgery 2Nd Edition Kirk N Gelatt All ChapterDocument67 paginiVeterinary Ophthalmic Surgery 2Nd Edition Kirk N Gelatt All Chaptermason.rempel179100% (2)
- 2ND Periodical Exam Sci 3Document3 pagini2ND Periodical Exam Sci 3Jasmin Llanes RocafortÎncă nu există evaluări
- 4 Contact LensesDocument17 pagini4 Contact LensesRaison D EtreÎncă nu există evaluări
- Anatomy Revisi KonsDocument28 paginiAnatomy Revisi KonsGun Gun GunawanÎncă nu există evaluări
- ENUCLEATIONDocument3 paginiENUCLEATIONTessa BingaroÎncă nu există evaluări
- How To Download Etextbook 978 0321989178 Introductory Statistics 10Th Edition by Neil A Weiss Ebook PDF Docx Kindle Full ChapterDocument36 paginiHow To Download Etextbook 978 0321989178 Introductory Statistics 10Th Edition by Neil A Weiss Ebook PDF Docx Kindle Full Chapterdonald.collins225100% (25)
- Optec 2300 RDocument55 paginiOptec 2300 Rjojors100% (1)
- Low Vision Aids: Visual Outcomes and Barriers in Children With Low VisionDocument4 paginiLow Vision Aids: Visual Outcomes and Barriers in Children With Low VisionshishichanÎncă nu există evaluări
- 05 Assignment IIIDocument13 pagini05 Assignment IIISubhashChandraMishraÎncă nu există evaluări
- Cmeseries 28Document88 paginiCmeseries 28ashishÎncă nu există evaluări
- SUN GAZING-processDocument7 paginiSUN GAZING-processsdms51Încă nu există evaluări
- Opto 11 85Document12 paginiOpto 11 85Sugi ArthaÎncă nu există evaluări
- Physics LightDocument107 paginiPhysics LightBlessing TshumaÎncă nu există evaluări
- Hunterlab ColorDocument47 paginiHunterlab ColorMd. Sazzadul IslamÎncă nu există evaluări
- Bio Module-02Document40 paginiBio Module-02XdxdÎncă nu există evaluări