S-ar putea să vă placă și
- Chart of The Acupuncture Meridian Clock PDFDocument10 paginiChart of The Acupuncture Meridian Clock PDFKesavadevÎncă nu există evaluări
- Acupuncture and ChiropracticDocument5 paginiAcupuncture and Chiropracticمحمد زبيدي نور الدين100% (1)
- Led Light Therapy GuideDocument23 paginiLed Light Therapy GuidePeter Freimann100% (4)
- Aculife BookletDocument99 paginiAculife BookletFaisal Raza67% (6)
- Body MeridiansDocument1 paginăBody MeridiansdoclozmakÎncă nu există evaluări
- Introduction to TCVM Diagnosis with Tongue and Pulse BasicsDocument22 paginiIntroduction to TCVM Diagnosis with Tongue and Pulse BasicsIngrid AtaydeÎncă nu există evaluări
- Basic Theories of Traditional Chinese Medicine PDFDocument194 paginiBasic Theories of Traditional Chinese Medicine PDFIon IonÎncă nu există evaluări
- Biomedical Acupuncture For Sports and Trauma Rehabilitation: Dry Needling TechniquesDocument6 paginiBiomedical Acupuncture For Sports and Trauma Rehabilitation: Dry Needling Techniquesbysinuti0% (1)
- Acupressure Points for Lowering High Blood PressureDocument2 paginiAcupressure Points for Lowering High Blood PressureRajul Gohil100% (1)
- ST 12Document1 paginăST 12ray72roÎncă nu există evaluări
- Pulse: Good Width at Medium Level, Regular, 78 BPM, Wiry On Right, Thin On LeftDocument11 paginiPulse: Good Width at Medium Level, Regular, 78 BPM, Wiry On Right, Thin On LeftHui YingÎncă nu există evaluări
- Master Cui's Four Flowers Points for Moxibustion TreatmentDocument4 paginiMaster Cui's Four Flowers Points for Moxibustion Treatmentgaetanscribd100% (1)
- Neck Training For Wrestlers-ClientDocument104 paginiNeck Training For Wrestlers-ClientIvan Medić100% (2)
- Acupuntura AlgoDocument6 paginiAcupuntura AlgoSergio SCÎncă nu există evaluări
- Shedding Light On The Practice of Moxibustion: Sana Throughout Latin America (Good Herb, Herb of Health) - Throughout 30Document6 paginiShedding Light On The Practice of Moxibustion: Sana Throughout Latin America (Good Herb, Herb of Health) - Throughout 30Daniel Medvedov - ELKENOS ABEÎncă nu există evaluări
- ScoliosisDocument9 paginiScoliosisexcalidorÎncă nu există evaluări
- 1996 Root and Branch Clinical ApplicationsDocument9 pagini1996 Root and Branch Clinical Applicationsdoktormin106Încă nu există evaluări
- The Silver Bullet The KOSA (Korean Orthodox Saahm Acupuncture) - NeedleLess AcupunctureDocument57 paginiThe Silver Bullet The KOSA (Korean Orthodox Saahm Acupuncture) - NeedleLess AcupuncturePowChoy83% (12)
- Understanding and Treating Hot Flashes in MenopauseDocument338 paginiUnderstanding and Treating Hot Flashes in MenopausePaco LaderaÎncă nu există evaluări
- Extra PointsDocument5 paginiExtra Pointsdelaney771Încă nu există evaluări
- Acupuncture Theory e TreatmentDocument11 paginiAcupuncture Theory e TreatmentCarlos Adam Yunus100% (1)
- Giovanni Maciocia 1945 - 2018Document2 paginiGiovanni Maciocia 1945 - 2018James GroblerÎncă nu există evaluări
- Obesity - Causes and Treatment OptionsDocument3 paginiObesity - Causes and Treatment OptionsPirasan Traditional Medicine CenterÎncă nu există evaluări
- TCMDocument49 paginiTCMdeemoney3Încă nu există evaluări
- Ren Mai - Conception Vessel The Sea of YinDocument18 paginiRen Mai - Conception Vessel The Sea of YinCarleta StanÎncă nu există evaluări
- RedbookDocument88 paginiRedbookNaresh MuttavarapuÎncă nu există evaluări
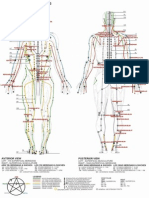
- Cutaneous Regions of the 14 Meridians MapDocument4 paginiCutaneous Regions of the 14 Meridians MapjjseguinÎncă nu există evaluări
- Course C Basic Theories of Acupuncture and MoxibustionDocument36 paginiCourse C Basic Theories of Acupuncture and MoxibustionGermey HoongÎncă nu există evaluări
- Babu's Notes On AcupunctureDocument14 paginiBabu's Notes On Acupuncturemailbabu100% (1)
- Sound and ResonanceDocument12 paginiSound and ResonanceHeart SoulÎncă nu există evaluări
- Foot AcupunctureDocument0 paginiFoot Acupuncturerasputin22Încă nu există evaluări
- Acupuncture Theory - OdtDocument2 paginiAcupuncture Theory - OdtAyyush RajalingaÎncă nu există evaluări
- RespiratoryDocument7 paginiRespiratoryThomas KearneyÎncă nu există evaluări
- Wood (Mu), Fire (Huo), Earth (Tu), Metal (Jin), Water (Shui)Document7 paginiWood (Mu), Fire (Huo), Earth (Tu), Metal (Jin), Water (Shui)Marina Rolla De LeoÎncă nu există evaluări
- 07 Caroline RadiceDocument7 pagini07 Caroline Radicetigerstyle1Încă nu există evaluări
- Traditional Chinese Medicine Resource Guide: Key Herbs, Formulas & HistoryDocument103 paginiTraditional Chinese Medicine Resource Guide: Key Herbs, Formulas & HistoryBrian LiÎncă nu există evaluări
- 3.14.15 Ymok Painmgmt LN ImagesDocument56 pagini3.14.15 Ymok Painmgmt LN ImagesSandar bandÎncă nu există evaluări
- The Big-Chart of Acupuncture Points: Source PointDocument1 paginăThe Big-Chart of Acupuncture Points: Source PointSelvakumarÎncă nu există evaluări
- TCM SampleDocument13 paginiTCM Sampleapi-3769511Încă nu există evaluări
- TCM Healthier LivingDocument21 paginiTCM Healthier LivingToffler NiemuthÎncă nu există evaluări
- TCM Acupuncture Theory - ... Points - Yin Yang HouseDocument2 paginiTCM Acupuncture Theory - ... Points - Yin Yang Houseabx5002Încă nu există evaluări
- Miyawaki Yuki Kuwahara Koei Hari Handbook of Traditional JapDocument23 paginiMiyawaki Yuki Kuwahara Koei Hari Handbook of Traditional Japкостя100% (1)
- Acupressure & Meridian Therapy: by Walter LastDocument10 paginiAcupressure & Meridian Therapy: by Walter LastEstela BenegildoÎncă nu există evaluări
- Su Jok, Twist Therapy AND Smile MeditationDocument7 paginiSu Jok, Twist Therapy AND Smile MeditationprateekÎncă nu există evaluări
- Biophotonics in The Infrared Spectral Range Reveal AcupunctureDocument4 paginiBiophotonics in The Infrared Spectral Range Reveal AcupunctureGalda Galdes100% (2)
- Two Acupuncture Styles for Painful Diabetic NeuropathyDocument7 paginiTwo Acupuncture Styles for Painful Diabetic NeuropathyAnonymous PFNzHoÎncă nu există evaluări
- 2017 Acupuncture For Chronic PainDocument49 pagini2017 Acupuncture For Chronic Painvera100% (1)
- A Skeptical Look at The AcuGraphDocument4 paginiA Skeptical Look at The AcuGraphhjsassoÎncă nu există evaluări
- Acupuncture in Medicine: A Metaphor for Therapeutic Transactions in History to the PresentDe la EverandAcupuncture in Medicine: A Metaphor for Therapeutic Transactions in History to the PresentÎncă nu există evaluări
- Clinical Practice - : Chronic Disease in Traditional Chinese MedicineDocument11 paginiClinical Practice - : Chronic Disease in Traditional Chinese MedicineScott KraemerÎncă nu există evaluări
- Health Communication in Traditional Chinese MedicineDe la EverandHealth Communication in Traditional Chinese MedicineÎncă nu există evaluări
- Respiratory Examination - Protected 1Document4 paginiRespiratory Examination - Protected 1anirudh811100% (1)
- Hijama CuppingDocument10 paginiHijama CuppingRancho Vaibhav GuptaÎncă nu există evaluări
- Cheng AcupunctureforWomenwithObesity PDFDocument13 paginiCheng AcupunctureforWomenwithObesity PDFAshari Fisio180% (1)
- Cupping TherapyDocument17 paginiCupping TherapyKalyan Chemist and druggistÎncă nu există evaluări
- TCM CatalogDocument16 paginiTCM CatalogNidhi RathodÎncă nu există evaluări
- Acupressure and Acupuncture: An Alternative TherapyDocument43 paginiAcupressure and Acupuncture: An Alternative Therapyhumag143Încă nu există evaluări
- Anesthetic Efficacy of Clove Oil and Its Impact On Hematological and Biochemical Changes in Channa Striatus (Bloch, 1793)Document9 paginiAnesthetic Efficacy of Clove Oil and Its Impact On Hematological and Biochemical Changes in Channa Striatus (Bloch, 1793)researchinbiologyÎncă nu există evaluări
- Acupressure: BackgroundDocument4 paginiAcupressure: BackgroundPrabhsimran SinghÎncă nu există evaluări
- 08152011-Article 0 PDFDocument2 pagini08152011-Article 0 PDFЕвгений ТополовскийÎncă nu există evaluări
- BooksDocument13 paginiBooksDoru Vrajitoru0% (1)
- Abdominal PalpationDocument11 paginiAbdominal PalpationDoctora SantanaÎncă nu există evaluări
- M.D. (Acu) SyllabusDocument5 paginiM.D. (Acu) SyllabusS Ve SuriyaÎncă nu există evaluări
- M.E.a.D. Report ComparisonsDocument1 paginăM.E.a.D. Report ComparisonsFaisal MadjidÎncă nu există evaluări
- Physiological Basis of Acupuncture TherapyDocument6 paginiPhysiological Basis of Acupuncture Therapydrak44Încă nu există evaluări
- Stroke Study 1994 PDFDocument5 paginiStroke Study 1994 PDFCarleta StanÎncă nu există evaluări
- Menopausal Syndrome FootDocument0 paginiMenopausal Syndrome Footrasputin22100% (1)
- Using Acupuncture Points To Eliminate Jet LagDocument5 paginiUsing Acupuncture Points To Eliminate Jet Lagsale18100% (1)
- Tennis Elbow GetDocument20 paginiTennis Elbow GetHeri DwiantoÎncă nu există evaluări
- Treatment of Hyperthyroidism: Western Medicine vs. Traditional Chinese MedicineDocument6 paginiTreatment of Hyperthyroidism: Western Medicine vs. Traditional Chinese MedicineShahul HameedÎncă nu există evaluări
- Compilation Conditions + FormulasDocument2 paginiCompilation Conditions + Formulaspeter911x0% (1)
- Acupuncture For The Treatment of Chronic Painful Peripheral Diabetic Neuropathy: A Long-Term StudyDocument7 paginiAcupuncture For The Treatment of Chronic Painful Peripheral Diabetic Neuropathy: A Long-Term StudyFernanda GiulianoÎncă nu există evaluări
- Lecture+03+Chinese+Medicine+in+the+Late+Imperial+Period+Part+I +song Jin Yuan+STUDENTSDocument15 paginiLecture+03+Chinese+Medicine+in+the+Late+Imperial+Period+Part+I +song Jin Yuan+STUDENTSyuxi4417Încă nu există evaluări
- TCM 1Document115 paginiTCM 1sai calderÎncă nu există evaluări
- Water-borne diseases: causes, prevention and controlDocument28 paginiWater-borne diseases: causes, prevention and controlEngr AliÎncă nu există evaluări
- YNM Part 2 - ExplainDocument61 paginiYNM Part 2 - ExplainCHAKRADHARA RAO100% (1)
- Tugas Farmakologi ToksikologiDocument55 paginiTugas Farmakologi ToksikologilucyanaÎncă nu există evaluări
- What Is AcupunctureDocument3 paginiWhat Is AcupunctureSreedhar PulipatiÎncă nu există evaluări
- The Neurovascular Bundle of The Anterior Compartment ofDocument30 paginiThe Neurovascular Bundle of The Anterior Compartment ofAnnapurna Bose100% (2)
- Review Article: Complementary and Alternative Medicine and Cardiovascular Disease: An Evidence-Based ReviewDocument8 paginiReview Article: Complementary and Alternative Medicine and Cardiovascular Disease: An Evidence-Based ReviewantoscriÎncă nu există evaluări
- A New Pulse Diagnostic Technique & EHF Therapy on Pulse PointsDocument2 paginiA New Pulse Diagnostic Technique & EHF Therapy on Pulse Pointsshaukijameel100% (1)
- Part Seven: Incite Strong Responses, The Fifth River: The Seven Rivers of Healing, With Susun WeedDocument23 paginiPart Seven: Incite Strong Responses, The Fifth River: The Seven Rivers of Healing, With Susun WeedIveri AuraÎncă nu există evaluări
- Brain Imaging AcupunctureDocument6 paginiBrain Imaging AcupunctureYoshua ViventiusÎncă nu există evaluări
- A Randomized Clinical Trial Comparing The Efficacy of Low-Level Laser Therapy (LLLT) and Laser Acupuncture Therapy (LAT) in Patients With Temporomandibular Disorders (Madani2019)Document12 paginiA Randomized Clinical Trial Comparing The Efficacy of Low-Level Laser Therapy (LLLT) and Laser Acupuncture Therapy (LAT) in Patients With Temporomandibular Disorders (Madani2019)monkeyhsuÎncă nu există evaluări
- Placebo Studies Ritual TheoryDocument10 paginiPlacebo Studies Ritual Theoryapi-443830029Încă nu există evaluări
- Physiotherapy and Acupuncture Practice in DenmarkDocument6 paginiPhysiotherapy and Acupuncture Practice in Denmarkbinglei chenÎncă nu există evaluări
- (Analysis On The Mechanism of Acupuncture Infrasound Energy in Treatment of Diseases) - PubMed - NCBIDocument1 pagină(Analysis On The Mechanism of Acupuncture Infrasound Energy in Treatment of Diseases) - PubMed - NCBIHeart SoulÎncă nu există evaluări
- Practice Exercise - Grade 10 Văn Unit 2. Your Body and You: Part I. PhoneticsDocument16 paginiPractice Exercise - Grade 10 Văn Unit 2. Your Body and You: Part I. Phoneticslqnam74Încă nu există evaluări