S-ar putea să vă placă și
- Iodide and Bromide Ions in Brackish Water, Seawater, and Brines D 3869 - 04Document12 paginiIodide and Bromide Ions in Brackish Water, Seawater, and Brines D 3869 - 04stevgonÎncă nu există evaluări
- FBC MNCS Service-, Error-, Infocodes ENDocument23 paginiFBC MNCS Service-, Error-, Infocodes ENDragos Stoian100% (1)
- Periodontal Treatment of Excessive Gingival DisplayDocument12 paginiPeriodontal Treatment of Excessive Gingival DisplayJuan Carlos CárcamoÎncă nu există evaluări
- White1997 Dental Calculus Formation EtcDocument16 paginiWhite1997 Dental Calculus Formation EtcJose Salas AdragnaÎncă nu există evaluări
- SOPDocument16 paginiSOPjerome marquezÎncă nu există evaluări
- CalculusDocument7 paginiCalculusFaikar Ardhan ArganagaraÎncă nu există evaluări
- (13C) The Role of Dental Calculus and Other Local Predisposing FactorsDocument9 pagini(13C) The Role of Dental Calculus and Other Local Predisposing FactorsNegrus StefanÎncă nu există evaluări
- Dental CalculusDocument70 paginiDental CalculusDUKUZIMANA CONCORDEÎncă nu există evaluări
- Content ServerDocument7 paginiContent ServerJUAN DIEGO DUARTE VILLARREALÎncă nu există evaluări
- Discussion 3Document33 paginiDiscussion 3navyaharitha nandinaÎncă nu există evaluări
- Calculus PresentationDocument62 paginiCalculus PresentationPiyusha Sharma100% (2)
- The Aetiology of Gingival RecessionDocument4 paginiThe Aetiology of Gingival RecessionshahidibrarÎncă nu există evaluări
- Combined Orthodontic - .Vdphjohjwbm5Sfbunfoupgb Q 1ptupsuipepoujd (Johjwbm3FdfttjpoDocument16 paginiCombined Orthodontic - .Vdphjohjwbm5Sfbunfoupgb Q 1ptupsuipepoujd (Johjwbm3FdfttjpobetziiÎncă nu există evaluări
- Prevalence, Location, and Patency of Accessory Canals in The Furcation Region of Permanent MolarsDocument6 paginiPrevalence, Location, and Patency of Accessory Canals in The Furcation Region of Permanent MolarsKathy YehÎncă nu există evaluări
- Tissue Response To Dental CariesDocument24 paginiTissue Response To Dental CariesGabriel Miloiu100% (1)
- Pal A To Gingival GrooveDocument5 paginiPal A To Gingival GrooveValonia IreneÎncă nu există evaluări
- Atlas de Endodoncia 2a Ed. (C. Stock Et Al, Hartcourt Brace 1996) VirgencitadelospxDocument276 paginiAtlas de Endodoncia 2a Ed. (C. Stock Et Al, Hartcourt Brace 1996) VirgencitadelospxLeidi Diana Marlenne100% (2)
- 2005 Gulavibala - Effects of Mechanical and Chemical Procedures On Root Canal SurfacesDocument20 pagini2005 Gulavibala - Effects of Mechanical and Chemical Procedures On Root Canal SurfacesCarlos San MartinÎncă nu există evaluări
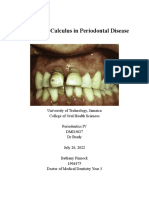
- Bethany Pinnock - Perio IV Final PaperDocument4 paginiBethany Pinnock - Perio IV Final PaperBethany PinnockÎncă nu există evaluări
- A Systematic Approach To Deep Caries Removal End PointsDocument13 paginiA Systematic Approach To Deep Caries Removal End PointsJosé Misael Aguilar FloresÎncă nu există evaluări
- The Complete Periodontal Examination (2004)Document12 paginiThe Complete Periodontal Examination (2004)fdsa1357Încă nu există evaluări
- Dental CalculusDocument10 paginiDental Calculusاحمد سلامÎncă nu există evaluări
- 44 PodjDocument8 pagini44 PodjTrefina PranaÎncă nu există evaluări
- Dental Calculus1hxDocument67 paginiDental Calculus1hxAyaÎncă nu există evaluări
- Newman Carranza's Clinical Periodonyology 11th Ed-Ublog TKDocument5 paginiNewman Carranza's Clinical Periodonyology 11th Ed-Ublog TKFahmi RexandyÎncă nu există evaluări
- Severe Gingival Recession Caused by Traumatic Occlusion and Mucogingival Stress: A Case ReportDocument8 paginiSevere Gingival Recession Caused by Traumatic Occlusion and Mucogingival Stress: A Case ReportSome TimeÎncă nu există evaluări
- Garib (2010) - Alveolar Bone Morphology Under The Perspective of The Computed Tomography. Defining The Biological Limits of Tooth Movement PDFDocument15 paginiGarib (2010) - Alveolar Bone Morphology Under The Perspective of The Computed Tomography. Defining The Biological Limits of Tooth Movement PDFIsmaelLouGomezÎncă nu există evaluări
- Periodontology 2000 - 2003 - DeSANCTIS - The Role of Resective Periodontal Surgery in The Treatment of Furcation DefectsDocument15 paginiPeriodontology 2000 - 2003 - DeSANCTIS - The Role of Resective Periodontal Surgery in The Treatment of Furcation Defectscarla lopezÎncă nu există evaluări
- Perio DR Maha Shukri: Furcation InvolvementDocument26 paginiPerio DR Maha Shukri: Furcation InvolvementYehya Al KhashabÎncă nu există evaluări
- Calculus Removal & Prevention of Its FormationDocument22 paginiCalculus Removal & Prevention of Its FormationsyamsaÎncă nu există evaluări
- Dayo AF, Et Al. Radiology of Dental Caries. Dental Clinics of North America. 2021Document19 paginiDayo AF, Et Al. Radiology of Dental Caries. Dental Clinics of North America. 2021miranda gitawÎncă nu există evaluări
- Lip Modification Procedures As An Adjunct To Improving Smile and Dental EstheticsDocument24 paginiLip Modification Procedures As An Adjunct To Improving Smile and Dental Estheticscmfvaldesr7Încă nu există evaluări
- Progressive Changes in The Pulpo DentinaDocument11 paginiProgressive Changes in The Pulpo Dentinaatzin espinozaÎncă nu există evaluări
- SaucerizationDocument12 paginiSaucerizationSaran NuiÎncă nu există evaluări
- Common Causes of Swelling in The Oral CavityDocument12 paginiCommon Causes of Swelling in The Oral CavityScribdÎncă nu există evaluări
- tmpB15C TMPDocument5 paginitmpB15C TMPFrontiersÎncă nu există evaluări
- Fixed Partial Dentures and Operative DentistryDocument6 paginiFixed Partial Dentures and Operative DentistryAlina AnechiteiÎncă nu există evaluări
- Odontogenic CystsDocument106 paginiOdontogenic Cystsريام الموسويÎncă nu există evaluări
- CalculusDocument36 paginiCalculusyogeshÎncă nu există evaluări
- Dental CalculusDocument5 paginiDental CalculusAbas HamzaÎncă nu există evaluări
- Corrected General 16.05Document33 paginiCorrected General 16.05Nia AdibÎncă nu există evaluări
- Pulp Space Anatomy and Access CavitiesDocument8 paginiPulp Space Anatomy and Access CavitiesMustafa SameerÎncă nu există evaluări
- Dental Calculus 1Document46 paginiDental Calculus 1AssssssÎncă nu există evaluări
- MtaDocument24 paginiMtadanidani_01Încă nu există evaluări
- Pubmed 9395117Document3 paginiPubmed 9395117Nabilaa PutriÎncă nu există evaluări
- Zucchelli 2006Document8 paginiZucchelli 2006Evan BlackwellÎncă nu există evaluări
- Original Articles: Rationale and Methods For Crown LengtheningDocument4 paginiOriginal Articles: Rationale and Methods For Crown LengtheningAna CernaianuÎncă nu există evaluări
- Course 7Document6 paginiCourse 7Tal ShvetsÎncă nu există evaluări
- Orthodontics andDocument9 paginiOrthodontics andSimona DobreÎncă nu există evaluări
- Jured BMDocument13 paginiJured BMSenomiya KeiÎncă nu există evaluări
- Short Cases NovDocument64 paginiShort Cases NovSoha Jan KhuhawarÎncă nu există evaluări
- William L. Chung Kurt Summersgill Mark Ochs: OdontogenicDocument18 paginiWilliam L. Chung Kurt Summersgill Mark Ochs: OdontogenicyosephineninaÎncă nu există evaluări
- Managing Discoloured Non-Vital Teeth: The Inside/Outside Bleaching TechniqueDocument8 paginiManaging Discoloured Non-Vital Teeth: The Inside/Outside Bleaching TechniqueJesus Manuel Lopez VidalÎncă nu există evaluări
- Diagnostic Test: Visual ExaminationDocument51 paginiDiagnostic Test: Visual ExaminationDr.O.R.GANESAMURTHIÎncă nu există evaluări
- Artigo 7Document25 paginiArtigo 7Júlia OliveiraÎncă nu există evaluări
- MR Debabrata DattaDocument2 paginiMR Debabrata DattaKaushik DuttaÎncă nu există evaluări
- Plaque and BiofilmDocument59 paginiPlaque and BiofilmGorremuchu Srinivas100% (2)
- (2005) Becker (Ea) - Current Theories of Crown ContourDocument9 pagini(2005) Becker (Ea) - Current Theories of Crown Contourgustavo.lopez.rocha1990Încă nu există evaluări
- Dental Caries - A Dynamic Disease ProcessDocument7 paginiDental Caries - A Dynamic Disease ProcessPratej KiranÎncă nu există evaluări
- Periodontal Root Coverage: An Evidence-Based Guide to Prognosis and TreatmentDe la EverandPeriodontal Root Coverage: An Evidence-Based Guide to Prognosis and TreatmentÎncă nu există evaluări
- Understanding Periodontitis: A Comprehensive Guide to Periodontal Disease for Dentists, Dental Hygienists and Dental PatientsDe la EverandUnderstanding Periodontitis: A Comprehensive Guide to Periodontal Disease for Dentists, Dental Hygienists and Dental PatientsÎncă nu există evaluări
- Free Electron TheoryDocument8 paginiFree Electron TheoryNeelam KapoorÎncă nu există evaluări
- Javanese PeopleDocument22 paginiJavanese PeopleDenisaÎncă nu există evaluări
- Ecall Vs NG EcallDocument6 paginiEcall Vs NG EcallTrần Văn DũngÎncă nu există evaluări
- Sap Ewm OverviewDocument11 paginiSap Ewm OverviewsachinÎncă nu există evaluări
- Para Lec CombinedDocument83 paginiPara Lec CombinedClent Earl Jason O. BascoÎncă nu există evaluări
- 01-20 Optical Multiplexer and Demultiplexer BoardDocument57 pagini01-20 Optical Multiplexer and Demultiplexer BoardDaler ShorahmonovÎncă nu există evaluări
- Gujral FCMDocument102 paginiGujral FCMcandiddreamsÎncă nu există evaluări
- Nomenclatura SKFDocument1 paginăNomenclatura SKFJuan José MeroÎncă nu există evaluări
- Water Filling MachineDocument15 paginiWater Filling Machinepallab D RozarioÎncă nu există evaluări
- Coding DecodingDocument21 paginiCoding DecodingAditya VermaÎncă nu există evaluări
- Mega StructuresDocument2 paginiMega StructuresSanthosh KumarÎncă nu există evaluări
- EXCEL For Pump DesignDocument2 paginiEXCEL For Pump Designkad-7Încă nu există evaluări
- Worksheet - 143760187HS-II, TUTORIAL ON CH-5Document14 paginiWorksheet - 143760187HS-II, TUTORIAL ON CH-5A MusaverÎncă nu există evaluări
- Bchem 455 - Module 3Document42 paginiBchem 455 - Module 3WilliamÎncă nu există evaluări
- MMW ReviewerDocument3 paginiMMW ReviewerMarcSaloj NeryÎncă nu există evaluări
- Karl MarxDocument4 paginiKarl Marxeirvine noah isidroÎncă nu există evaluări
- Asme b16-25Document22 paginiAsme b16-25JamesÎncă nu există evaluări
- Practice For Mounting Buses & Joints-374561Document11 paginiPractice For Mounting Buses & Joints-374561a_sengar1Încă nu există evaluări
- Parameters Identification of Induction Motor Model BasedDocument10 paginiParameters Identification of Induction Motor Model Basedretrueke1170Încă nu există evaluări
- c270 KW NTA855G2 60 HZDocument31 paginic270 KW NTA855G2 60 HZAhmad El KhatibÎncă nu există evaluări
- ASME Pressue Vessel ExampleDocument271 paginiASME Pressue Vessel ExamplesavanchandranÎncă nu există evaluări
- Asme Code Sec Ix Ma Appe 2004Document3 paginiAsme Code Sec Ix Ma Appe 2004Guillermo CamachoÎncă nu există evaluări
- Aquaculture Scoop May IssueDocument20 paginiAquaculture Scoop May IssueAquaculture ScoopÎncă nu există evaluări
- PANASONIC - WebCam-TQZJ402 - TY-CC20W PDFDocument188 paginiPANASONIC - WebCam-TQZJ402 - TY-CC20W PDF123anthonyÎncă nu există evaluări
- Presentation AcetanilideDocument22 paginiPresentation AcetanilideNovitasarii JufriÎncă nu există evaluări
- Kaged Muscle Magazine Issue 1Document41 paginiKaged Muscle Magazine Issue 1hashimhafiz1100% (1)
- Diagnostic Imaging of The Pharynx and Esophagus: Key PointsDocument33 paginiDiagnostic Imaging of The Pharynx and Esophagus: Key PointsChutcharwan JintasoponÎncă nu există evaluări