S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- 81.4. RESCUE BOAT 4.1 - RSQ - 450 - GA - Operation - Maintenance - ManualDocument40 pagini81.4. RESCUE BOAT 4.1 - RSQ - 450 - GA - Operation - Maintenance - Manualwoki hoj0% (1)
- What Is Difference Between Maritime Survey N InspectionDocument1 paginăWhat Is Difference Between Maritime Survey N InspectionAjay SinghÎncă nu există evaluări
- Di 001 Contractor Ship Specifications Rev BDocument264 paginiDi 001 Contractor Ship Specifications Rev Bmaria_bustelo_2Încă nu există evaluări
- Ics Reading List 2016 WebDocument24 paginiIcs Reading List 2016 WebChristos AdÎncă nu există evaluări
- Course Specs Mar Law BSMT CHEDDocument63 paginiCourse Specs Mar Law BSMT CHEDjutester100% (1)
- Fundamentals of Plate TectonicsDocument5 paginiFundamentals of Plate TectonicsAjay SinghÎncă nu există evaluări
- MMD Ques - SSEMM - MP1Document9 paginiMMD Ques - SSEMM - MP1Ajay SinghÎncă nu există evaluări
- Fundamentals of Plate TectonicsDocument5 paginiFundamentals of Plate TectonicsAjay SinghÎncă nu există evaluări
- Ship Waves in ChannelDocument25 paginiShip Waves in ChannelAjay SinghÎncă nu există evaluări
- Geology and OceanographyDocument1 paginăGeology and OceanographyAjay Singh100% (1)
- TidesDocument36 paginiTidesAjay SinghÎncă nu există evaluări
- Emergency Towing Procedures Required For All ShipsDocument2 paginiEmergency Towing Procedures Required For All ShipsAjay Singh100% (1)
- The Apparent Solar TimeDocument3 paginiThe Apparent Solar TimeAjay SinghÎncă nu există evaluări
- Fundamentals of Plate TectonicsDocument5 paginiFundamentals of Plate TectonicsAjay SinghÎncă nu există evaluări
- B SC (Nautical)Document161 paginiB SC (Nautical)Ajay SinghÎncă nu există evaluări
- BL204 Radio SystemsDocument8 paginiBL204 Radio SystemsAjay SinghÎncă nu există evaluări
- ASM June 2019 ISM ManualDocument10 paginiASM June 2019 ISM ManualAjay Singh100% (1)
- Indian Holiday ResortsDocument4 paginiIndian Holiday ResortsAjay SinghÎncă nu există evaluări
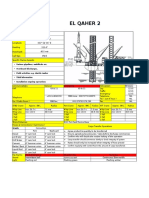
- ElQaher 2 Data CardDocument1 paginăElQaher 2 Data CardAjay SinghÎncă nu există evaluări
- Technical Specification DP SystemDocument48 paginiTechnical Specification DP SystemAjay SinghÎncă nu există evaluări
- Ship TermsDocument30 paginiShip TermsAjay SinghÎncă nu există evaluări
- Manual Resuscitator InstDocument7 paginiManual Resuscitator InstAjay SinghÎncă nu există evaluări
- First Aid KitDocument1 paginăFirst Aid KitAjay SinghÎncă nu există evaluări
- DrillingBasics English Version English NY 2008Document76 paginiDrillingBasics English Version English NY 2008Ajay SinghÎncă nu există evaluări
- Phasei&II Syllabus 111010Document30 paginiPhasei&II Syllabus 111010He SheÎncă nu există evaluări
- Draught Survey BlankDocument3 paginiDraught Survey BlankThyago de LellysÎncă nu există evaluări
- Draught Survey BlankDocument3 paginiDraught Survey BlankThyago de LellysÎncă nu există evaluări
- Anchoring and What Precautions To TakeDocument2 paginiAnchoring and What Precautions To Takevikrami100% (2)
- Procedure For Transmiting Designated VHF DSC Distress Alert From FurunoDocument1 paginăProcedure For Transmiting Designated VHF DSC Distress Alert From FurunoAjay SinghÎncă nu există evaluări
- Equipment No Sg01 Aldis LampDocument2 paginiEquipment No Sg01 Aldis LampAjay SinghÎncă nu există evaluări
- Equipment No 25 & 26Document2 paginiEquipment No 25 & 26Ajay SinghÎncă nu există evaluări
- EQUIPMENT No NA12 Speed Log RepeaterDocument2 paginiEQUIPMENT No NA12 Speed Log RepeaterAjay SinghÎncă nu există evaluări
- Equipment No Na01 RadarDocument2 paginiEquipment No Na01 RadarAjay SinghÎncă nu există evaluări
- Equipment No Na11 Speed LogDocument2 paginiEquipment No Na11 Speed LogAjay SinghÎncă nu există evaluări
- KM ECDIS Compatibility OverviewDocument13 paginiKM ECDIS Compatibility OverviewClarence PieterszÎncă nu există evaluări
- ISPS Code 2003Document137 paginiISPS Code 2003Condulimazi Paul100% (2)
- Saep 32Document19 paginiSaep 32OMER ELFADILÎncă nu există evaluări
- (PMMRR 1997) - Philippine Merchant Marine Rules and RegulationsDocument114 pagini(PMMRR 1997) - Philippine Merchant Marine Rules and Regulationsranchdressing104Încă nu există evaluări
- International and Inland (US) Rules of The RoadDocument224 paginiInternational and Inland (US) Rules of The RoadbrubruniÎncă nu există evaluări
- Portable Fire ExtinguishersDocument10 paginiPortable Fire Extinguishersemrealacayir100% (1)
- STCW-95: A Guide For Seafarers: International Transport Workers FederationDocument88 paginiSTCW-95: A Guide For Seafarers: International Transport Workers Federationmingo622Încă nu există evaluări
- Pilot Ladder SafetyDocument59 paginiPilot Ladder SafetyYamani100% (1)
- Reporting Format: Format of Ship ReportDocument4 paginiReporting Format: Format of Ship ReportIhwan AsrulÎncă nu există evaluări
- Biofouling ManagementDocument20 paginiBiofouling ManagementMehmet AliÎncă nu există evaluări
- Wreck Removal Certificate - FlagDocument1 paginăWreck Removal Certificate - FlagSherry GodwinÎncă nu există evaluări
- Model Ship To Ship Transfer Operations PlanDocument47 paginiModel Ship To Ship Transfer Operations PlanAnkit VyasÎncă nu există evaluări
- Oral SetsDocument80 paginiOral SetsRao Durga75% (4)
- NI 597 - Additional Class Notation SEEMP (Ship Energy Efficiency Management Plan)Document20 paginiNI 597 - Additional Class Notation SEEMP (Ship Energy Efficiency Management Plan)youngfpÎncă nu există evaluări
- Orals by Karthik Revision Function 3 Chef MateDocument75 paginiOrals by Karthik Revision Function 3 Chef MateAnkit MauryaÎncă nu există evaluări
- MGN 284 - Fumigated CargoesDocument3 paginiMGN 284 - Fumigated Cargoesaakash9090Încă nu există evaluări
- MSC.1-Circ.1042 - List of Contents of The Emergency Medical KitBagln and Medical Consideration PDFDocument7 paginiMSC.1-Circ.1042 - List of Contents of The Emergency Medical KitBagln and Medical Consideration PDFJeet SinghÎncă nu există evaluări
- Revised Guidelines For Formal Safety Assessment (Fsa) - Msc-Mepc 2-Circ 12-Rev 2Document71 paginiRevised Guidelines For Formal Safety Assessment (Fsa) - Msc-Mepc 2-Circ 12-Rev 2Martin NiÎncă nu există evaluări
- 125 Ton AHTSSV SpecificationDocument86 pagini125 Ton AHTSSV SpecificationChakma NhikiÎncă nu există evaluări
- National Ballast Water Management Requirements: 22 March 2019Document46 paginiNational Ballast Water Management Requirements: 22 March 2019กัปตัน นเรศ สิงห์สอาดÎncă nu există evaluări
- MSC.1-Circ.1182 - Guide To Recovery Techniques (Secretariat)Document21 paginiMSC.1-Circ.1182 - Guide To Recovery Techniques (Secretariat)RihardsÎncă nu există evaluări
- MEPC 75-3-3 - Comments On The Draft Amendments To The MARPOL Annex VI (Republic of Korea) PDFDocument6 paginiMEPC 75-3-3 - Comments On The Draft Amendments To The MARPOL Annex VI (Republic of Korea) PDFkrzysztofeles5Încă nu există evaluări
- IMO Instruments - Summary - ReportDocument4 paginiIMO Instruments - Summary - ReportMithran DirÎncă nu există evaluări
- 5470.43.530NR - 2013-07 - Coating PerformanceDocument22 pagini5470.43.530NR - 2013-07 - Coating PerformanceMohamed Mostafa100% (1)
- Marine Law and Management An Introduction (DF0LJ34)Document145 paginiMarine Law and Management An Introduction (DF0LJ34)Merchant NavyÎncă nu există evaluări
- 61 Mepc ReportDocument211 pagini61 Mepc ReportGeorgios PapakostasÎncă nu există evaluări