S-ar putea să vă placă și
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- 5 Natural Sore Throat RemediesDocument5 pagini5 Natural Sore Throat Remedieslisa smithis100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Acalculous Cholecystitis CaseDocument35 paginiAcalculous Cholecystitis CaseSaada Enok MedtamakÎncă nu există evaluări
- Flight School BundleDocument43 paginiFlight School BundleyoyoÎncă nu există evaluări
- Clinical Algorithms in General Surgery PDFDocument786 paginiClinical Algorithms in General Surgery PDFLaura Campaña100% (5)
- CS1 Epoxy Curing AgentsDocument21 paginiCS1 Epoxy Curing AgentsAlptekin100% (1)
- Electronic Data ProcessingDocument8 paginiElectronic Data ProcessingJayvee Puntalba Calinog100% (1)
- VW Golf 8 Variant WD EngDocument664 paginiVW Golf 8 Variant WD EngLakhdar BouchenakÎncă nu există evaluări
- Social InequalityDocument55 paginiSocial InequalityJayvee Puntalba Calinog100% (1)
- Leonard Peikoff-Introduction To LogicDocument20 paginiLeonard Peikoff-Introduction To Logicbursa07Încă nu există evaluări
- Summary (Adjuncts)Document2 paginiSummary (Adjuncts)Ngọc MinhÎncă nu există evaluări
- Date Time Record Name: Calinog, Jayvee P. Section:IS41-2Document4 paginiDate Time Record Name: Calinog, Jayvee P. Section:IS41-2Jayvee Puntalba CalinogÎncă nu există evaluări
- Date Time Record Name: Calinog, Jayvee P. Section:IS41-2Document5 paginiDate Time Record Name: Calinog, Jayvee P. Section:IS41-2Jayvee Puntalba CalinogÎncă nu există evaluări
- Date Time Record Name: Calinog, Jayvee P. Section:IS41-2Document4 paginiDate Time Record Name: Calinog, Jayvee P. Section:IS41-2Jayvee Puntalba CalinogÎncă nu există evaluări
- Jayvee Calinog OJT AMA Time StampDocument4 paginiJayvee Calinog OJT AMA Time StampJayvee Puntalba CalinogÎncă nu există evaluări
- Lloyd SanchezDocument6 paginiLloyd SanchezJayvee Puntalba CalinogÎncă nu există evaluări
- Test PrintDocument1 paginăTest PrintJayvee Puntalba CalinogÎncă nu există evaluări
- Attendance - Small SundayDocument1 paginăAttendance - Small SundayJayvee Puntalba CalinogÎncă nu există evaluări
- Smaple ExamDocument16 paginiSmaple ExamJayvee Puntalba CalinogÎncă nu există evaluări
- 10 Isim E-ExamDocument11 pagini10 Isim E-ExamJayvee Puntalba CalinogÎncă nu există evaluări
- Network TopologyDocument7 paginiNetwork TopologyJayvee Puntalba CalinogÎncă nu există evaluări
- GamblingDocument14 paginiGamblingJayvee Puntalba CalinogÎncă nu există evaluări
- The Top 100 Common Usage ProblemsDocument4 paginiThe Top 100 Common Usage ProblemsJayvee Puntalba Calinog100% (2)
- FMDS0289 Pipe Friction LossDocument64 paginiFMDS0289 Pipe Friction Lossdaniela hritucÎncă nu există evaluări
- World Wide Emission Free E-Motercycle ProjectDocument20 paginiWorld Wide Emission Free E-Motercycle ProjectAkshay SharmaÎncă nu există evaluări
- Afcat Question Paper 01-2014 PDFDocument10 paginiAfcat Question Paper 01-2014 PDFTuhin AzadÎncă nu există evaluări
- How Hydraulic Valve Lifters WorkDocument1 paginăHow Hydraulic Valve Lifters WorkSanket Sabale100% (1)
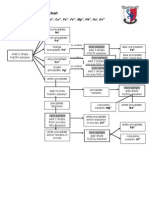
- Testing For Cations Flow ChartDocument2 paginiTesting For Cations Flow Chartapi-252561013Încă nu există evaluări
- Psicologia BuenisimoDocument6 paginiPsicologia BuenisimoSophieÎncă nu există evaluări
- 1101259L 580.752830 Pressure Washer ManualDocument64 pagini1101259L 580.752830 Pressure Washer Manualgork1roguesÎncă nu există evaluări
- 6 Instrumentation PDFDocument144 pagini6 Instrumentation PDFWanderley MandruzatoÎncă nu există evaluări
- Lead and Manage People TTLMDocument41 paginiLead and Manage People TTLMHenok Mehari100% (1)
- Assessment 2 Vital Signs Normal ValuesDocument4 paginiAssessment 2 Vital Signs Normal Valuesthannikkotte12345Încă nu există evaluări
- CV Mary Mugo 2017Document4 paginiCV Mary Mugo 2017Mary Wanja MugoÎncă nu există evaluări
- Total Parenteral NutritionDocument8 paginiTotal Parenteral NutritionTemiloluwa AdeyemiÎncă nu există evaluări
- Convecc Ao Forc Ada Externa: Vicente Luiz ScalonDocument18 paginiConvecc Ao Forc Ada Externa: Vicente Luiz ScalonMaria VitóriaÎncă nu există evaluări
- Dingenen 2017Document14 paginiDingenen 2017pedro.coleffÎncă nu există evaluări
- Static Fluid: It Is Mass Per Unit Volume at Certain TemperatureDocument11 paginiStatic Fluid: It Is Mass Per Unit Volume at Certain TemperatureMohamed El-GoharyÎncă nu există evaluări
- Big BazaarDocument6 paginiBig BazaaraniketsangodcarÎncă nu există evaluări
- User Manual 4372070Document80 paginiUser Manual 4372070EDENILSON CORDEIROÎncă nu există evaluări
- VEIKK A15PRO Instruction Manual 0714Document20 paginiVEIKK A15PRO Instruction Manual 0714Corny777 UwUÎncă nu există evaluări
- Standardization 1 PDFDocument7 paginiStandardization 1 PDFmazharul HasanÎncă nu există evaluări
- What Is A Walkable Place The Walkability Debate inDocument20 paginiWhat Is A Walkable Place The Walkability Debate inBADR HAMDAN ALATEBEÎncă nu există evaluări
- Exam G-9 CookeryDocument5 paginiExam G-9 Cookeryaileenarcabal01Încă nu există evaluări
- Weigh Bridge Miscellaneous Items DetailsDocument1 paginăWeigh Bridge Miscellaneous Items DetailsChandan RayÎncă nu există evaluări