S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Homebuilding - Renovating-UltimateDesignBuildGuideDocument60 paginiHomebuilding - Renovating-UltimateDesignBuildGuideverivtudawÎncă nu există evaluări
- False CeilingDocument70 paginiFalse CeilingBharti Sikri93% (15)
- PreviewpdfDocument50 paginiPreviewpdfMarcosGouvea100% (1)
- Dental CompositeDocument60 paginiDental CompositelalitboruahÎncă nu există evaluări
- Dental CompositeDocument60 paginiDental CompositelalitboruahÎncă nu există evaluări
- Periodontal IndicesDocument29 paginiPeriodontal IndicesFachrul Latif DentistÎncă nu există evaluări
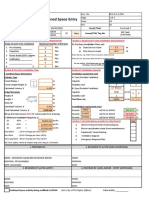
- Ventilation Plan For Confined Space EntryDocument9 paginiVentilation Plan For Confined Space EntryMohamad Nazmi Mohamad Rafian100% (1)
- Price ListDocument30 paginiPrice ListFachrul Latif DentistÎncă nu există evaluări
- Persatuan Dokter Gigi IndonesiaDocument1 paginăPersatuan Dokter Gigi IndonesiaFachrul Latif DentistÎncă nu există evaluări
- Pedoman Kaji BandingDocument17 paginiPedoman Kaji BandingFachrul Latif DentistÎncă nu există evaluări
- Arch Bar and Ernst Ligature for Mandibular Fracture FixationDocument28 paginiArch Bar and Ernst Ligature for Mandibular Fracture FixationFachrul Latif DentistÎncă nu există evaluări
- Persatuan Dokter Gigi IndonesiaDocument1 paginăPersatuan Dokter Gigi IndonesiaFachrul Latif DentistÎncă nu există evaluări
- Price List DENTAL JAYA Dental Supply PDFDocument30 paginiPrice List DENTAL JAYA Dental Supply PDFFachrul Latif DentistÎncă nu există evaluări
- DENTAL UNIT FUNCTIONS AND COMPONENTSDocument186 paginiDENTAL UNIT FUNCTIONS AND COMPONENTSFachrul Latif DentistÎncă nu există evaluări
- Price List CAB Dental 2016Document12 paginiPrice List CAB Dental 2016Fachrul Latif DentistÎncă nu există evaluări
- 535321Document17 pagini535321Fachrul Latif DentistÎncă nu există evaluări
- JIndianSocPedodPrevDent293273-1253582 032855Document5 paginiJIndianSocPedodPrevDent293273-1253582 032855Fachrul Latif DentistÎncă nu există evaluări
- Class I I I Treatment With Ske Let A AnchorageDocument12 paginiClass I I I Treatment With Ske Let A AnchorageFachrul Latif DentistÎncă nu există evaluări
- KonserDocument5 paginiKonserFachrul Latif DentistÎncă nu există evaluări
- Jpis 41 279Document6 paginiJpis 41 279Fachrul Latif DentistÎncă nu există evaluări
- Jop 2010 090646Document6 paginiJop 2010 090646Fachrul Latif DentistÎncă nu există evaluări
- Jop 2009 097001Document12 paginiJop 2009 097001Fachrul Latif DentistÎncă nu există evaluări
- Submandibular Displacement of A Mandibular Third Molar Root During Extraction: A Case ReportDocument3 paginiSubmandibular Displacement of A Mandibular Third Molar Root During Extraction: A Case ReportFachrul Latif DentistÎncă nu există evaluări
- Higher Algebra - Hall & KnightDocument593 paginiHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- DENTAL UNIT FUNCTIONS AND COMPONENTSDocument186 paginiDENTAL UNIT FUNCTIONS AND COMPONENTSFachrul Latif DentistÎncă nu există evaluări
- Infeksi Mukosa MulutDocument165 paginiInfeksi Mukosa MulutRistoria Sps SimboNaÎncă nu există evaluări
- Higher Algebra - Hall & KnightDocument593 paginiHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Higher Algebra - Hall & KnightDocument593 paginiHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Higher Algebra - Hall & KnightDocument593 paginiHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Usg Sheetrock® Brand Acoustical SealantDocument3 paginiUsg Sheetrock® Brand Acoustical SealantHoracio PadillaÎncă nu există evaluări
- Flaechendicht k435 de 0216 0 Eng ScreenDocument2 paginiFlaechendicht k435 de 0216 0 Eng ScreenAlexandru IonescuÎncă nu există evaluări
- Suggested For You: 15188 5 Years Ago 20:50Document1 paginăSuggested For You: 15188 5 Years Ago 20:50DeevenÎncă nu există evaluări
- Product PlanningDocument23 paginiProduct PlanningGrechen CabusaoÎncă nu există evaluări
- Industrial Visit Report - 08 09 2018Document11 paginiIndustrial Visit Report - 08 09 2018HARIKRISHNA MÎncă nu există evaluări
- Area Manager ChecklistDocument7 paginiArea Manager ChecklistUtkarsh RaiÎncă nu există evaluări
- E-Governance in KeralaDocument10 paginiE-Governance in KeralaRahmath SafeenaÎncă nu există evaluări
- Languages and CommunicationDocument17 paginiLanguages and CommunicationDERICK REBAYÎncă nu există evaluări
- JURNAL PENCONG IJAS FixDocument12 paginiJURNAL PENCONG IJAS Fixmasri ridwanÎncă nu există evaluări
- Six Sigma MotorolaDocument3 paginiSix Sigma MotorolarafaÎncă nu există evaluări
- MMA Electrode ClassificationDocument3 paginiMMA Electrode ClassificationRathnakrajaÎncă nu există evaluări
- 9608/21/M/J/15 © Ucles 2015Document57 pagini9608/21/M/J/15 © Ucles 2015Asilbek AshurovÎncă nu există evaluări
- Line BalancingDocument21 paginiLine Balancingarno6antonio6spinaÎncă nu există evaluări
- AssignmentDocument15 paginiAssignmentWahab MirzaÎncă nu există evaluări
- Perfect Secrecy: Chester Rebeiro IIT MadrasDocument50 paginiPerfect Secrecy: Chester Rebeiro IIT MadrasDr. Jayanthi V.S.Încă nu există evaluări
- Sae Technical Paper Series 2015-36-0353: Static and Dynamic Analysis of A Chassis of A Prototype CarDocument12 paginiSae Technical Paper Series 2015-36-0353: Static and Dynamic Analysis of A Chassis of A Prototype CarGanesh KCÎncă nu există evaluări
- Sick GM31Document54 paginiSick GM31Magdy SalehÎncă nu există evaluări
- The Art of Grooming - 230301 - 222106Document61 paginiThe Art of Grooming - 230301 - 222106ConstantinÎncă nu există evaluări
- Leadership EthiqueDocument16 paginiLeadership EthiqueNOURDINE EZZALMADIÎncă nu există evaluări
- Bio-Climatic Tower/Eco-Tower: Bachelor of ArchitectureDocument12 paginiBio-Climatic Tower/Eco-Tower: Bachelor of ArchitectureZorawar Singh Basur67% (3)
- Ternary Phase Diagram Guided Question 1 PDFDocument1 paginăTernary Phase Diagram Guided Question 1 PDFLuci FernÎncă nu există evaluări
- Stress Amongst Healthcare Professionals and Migrant Workers During Covid-19 PandemicDocument6 paginiStress Amongst Healthcare Professionals and Migrant Workers During Covid-19 PandemicIJAR JOURNALÎncă nu există evaluări
- Project Synopsis: "Employee Motivation at Syndicate Bank"Document5 paginiProject Synopsis: "Employee Motivation at Syndicate Bank"SubhamSahaÎncă nu există evaluări
- SNS Bank XS0382843802Document7 paginiSNS Bank XS0382843802Southey CapitalÎncă nu există evaluări
- Air CasterDocument25 paginiAir CasterPrabir Kumar Pati100% (1)
- Job Order Costing ExplainedDocument43 paginiJob Order Costing ExplainedZovia Lucio100% (1)