S-ar putea să vă placă și
- Effects of an Inclusion Professional Development Model on Inclusion Knowledge and Perceptions of Regular Middle School EducatorsDe la EverandEffects of an Inclusion Professional Development Model on Inclusion Knowledge and Perceptions of Regular Middle School EducatorsÎncă nu există evaluări
- Well-Child Care in Infancy: Promoting Readiness for LifeDe la EverandWell-Child Care in Infancy: Promoting Readiness for LifeÎncă nu există evaluări
- Perkins Activity and Resource Guide - Chapter 4: Functional Academics: Second Edition: Revised and UpdatedDe la EverandPerkins Activity and Resource Guide - Chapter 4: Functional Academics: Second Edition: Revised and UpdatedÎncă nu există evaluări
- Multi-Subject: Teachers of Childhood (Gr. 2–6): Passbooks Study GuideDe la EverandMulti-Subject: Teachers of Childhood (Gr. 2–6): Passbooks Study GuideÎncă nu există evaluări
- Alternate Assessment of Students with Significant Cognitive Disabilities: A Research ReportDe la EverandAlternate Assessment of Students with Significant Cognitive Disabilities: A Research ReportÎncă nu există evaluări
- The Social Validity Manual: A Guide to Subjective Evaluation of Behavior InterventionsDe la EverandThe Social Validity Manual: A Guide to Subjective Evaluation of Behavior InterventionsÎncă nu există evaluări
- Text InSPECtion on the Core: Close Reading Strategies for Uncovering Informational TextDe la EverandText InSPECtion on the Core: Close Reading Strategies for Uncovering Informational TextÎncă nu există evaluări
- The Teacher's Guide to Intervention and Inclusive Education: 1000+ Strategies to Help ALL Students Succeed!De la EverandThe Teacher's Guide to Intervention and Inclusive Education: 1000+ Strategies to Help ALL Students Succeed!Încă nu există evaluări
- A Progressive Approach to Applied Behavior Analysis: The Autism Partnership MethodDe la EverandA Progressive Approach to Applied Behavior Analysis: The Autism Partnership MethodÎncă nu există evaluări
- Autism: A Practical Guide for ParentsDe la EverandAutism: A Practical Guide for ParentsÎncă nu există evaluări
- Alaska's Children's House: Building Essential Skills, Independent Thinking, and CharacterDe la EverandAlaska's Children's House: Building Essential Skills, Independent Thinking, and CharacterÎncă nu există evaluări
- Triumph: A Curriculum for All Schools and UniversitiesDe la EverandTriumph: A Curriculum for All Schools and UniversitiesÎncă nu există evaluări
- What Successful Schools Do to Involve Families: 55 Partnership StrategiesDe la EverandWhat Successful Schools Do to Involve Families: 55 Partnership StrategiesÎncă nu există evaluări
- Early Science Education – Goals and Process-Related Quality Criteria for Science TeachingDe la EverandEarly Science Education – Goals and Process-Related Quality Criteria for Science TeachingEvaluare: 5 din 5 stele5/5 (1)
- Implementing RtI with Gifted Students: Service Models, Trends, and IssuesDe la EverandImplementing RtI with Gifted Students: Service Models, Trends, and IssuesEvaluare: 4.5 din 5 stele4.5/5 (6)
- Designing Teaching Strategies: An Applied Behavior Analysis Systems ApproachDe la EverandDesigning Teaching Strategies: An Applied Behavior Analysis Systems ApproachEvaluare: 4.5 din 5 stele4.5/5 (1)
- Handbook of Student Engagement Interventions: Working with Disengaged StudentsDe la EverandHandbook of Student Engagement Interventions: Working with Disengaged StudentsJennifer A. FredricksEvaluare: 5 din 5 stele5/5 (2)
- The QIAT Companion: A Just-in-Time Resource for Implementing the Quality Indicators for Assistive TechnologyDe la EverandThe QIAT Companion: A Just-in-Time Resource for Implementing the Quality Indicators for Assistive TechnologyÎncă nu există evaluări
- The School-Home Connection: Forging Positive Relationships with ParentsDe la EverandThe School-Home Connection: Forging Positive Relationships with ParentsÎncă nu există evaluări
- Cognitive and Behavioral Interventions in the Schools: Integrating Theory and Research into PracticeDe la EverandCognitive and Behavioral Interventions in the Schools: Integrating Theory and Research into PracticeRosemary FlanaganÎncă nu există evaluări
- Program evaluation Complete Self-Assessment GuideDe la EverandProgram evaluation Complete Self-Assessment GuideÎncă nu există evaluări
- Introduction to Curriculum Design in Gifted EducationDe la EverandIntroduction to Curriculum Design in Gifted EducationEvaluare: 4.5 din 5 stele4.5/5 (3)
- Access to Life Science: Investigation Starters for Preschool, Kindergarten and the Primary GradesDe la EverandAccess to Life Science: Investigation Starters for Preschool, Kindergarten and the Primary GradesÎncă nu există evaluări
- Relationship Development Intervention Second EditionDe la EverandRelationship Development Intervention Second EditionEvaluare: 5 din 5 stele5/5 (1)
- Ecological Assessment of Child Problem Behavior: A Clinical Package for Home, School, and Institutional Settings: Pergamon General Psychology SeriesDe la EverandEcological Assessment of Child Problem Behavior: A Clinical Package for Home, School, and Institutional Settings: Pergamon General Psychology SeriesÎncă nu există evaluări
- Empowering Parents & Teachers: How Parents and Teachers Can Develop Collaborative PartnershipsDe la EverandEmpowering Parents & Teachers: How Parents and Teachers Can Develop Collaborative PartnershipsÎncă nu există evaluări
- Conceptual Frameworks for Giftedness and Talent Development: Enduring Theories and Comprehensive Models in Gifted EducationDe la EverandConceptual Frameworks for Giftedness and Talent Development: Enduring Theories and Comprehensive Models in Gifted EducationÎncă nu există evaluări
- Assignment 3 Final Assignment Jake DowsettDocument7 paginiAssignment 3 Final Assignment Jake Dowsettapi-321376162Încă nu există evaluări
- Edu-690 Action Research PaperDocument27 paginiEdu-690 Action Research Paperapi-240639978Încă nu există evaluări
- Running Head: Reducing Disruptive Behavior: A Behavioral Intervention PlanDocument32 paginiRunning Head: Reducing Disruptive Behavior: A Behavioral Intervention Planapi-270220817Încă nu există evaluări
- Behaviorism PageDocument4 paginiBehaviorism Pageapi-270013525Încă nu există evaluări
- Diversity and Complexity in The ClassroomDocument11 paginiDiversity and Complexity in The ClassroomGiavannaMÎncă nu există evaluări
- Mtss PDDocument41 paginiMtss PDapi-543254726Încă nu există evaluări
- Expressive Language (Using Words and Language) : Print PDFDocument8 paginiExpressive Language (Using Words and Language) : Print PDFNico Corporal CañaveralÎncă nu există evaluări
- Pico FinalDocument11 paginiPico Finalapi-282751948Încă nu există evaluări
- Response To InterventionDocument11 paginiResponse To Interventionapi-548326746Încă nu există evaluări
- A Culturally-Inclusive Classroom EnvironmentDocument3 paginiA Culturally-Inclusive Classroom EnvironmentAlexana Bi VieÎncă nu există evaluări
- Effective Speech Language PathologyDocument173 paginiEffective Speech Language PathologyLucas Gandy100% (1)
- Diversity Lesson Plan TemplateDocument6 paginiDiversity Lesson Plan Templateapi-285015723Încă nu există evaluări
- The Role of Teacher To Address Issues of Disruptive Behaviour of Student Learners in Mathematics Classrooms - A Study in The Sri Lankan ContextDocument22 paginiThe Role of Teacher To Address Issues of Disruptive Behaviour of Student Learners in Mathematics Classrooms - A Study in The Sri Lankan ContextGlobal Research and Development ServicesÎncă nu există evaluări
- Inclusive Education Assignment 2 Case StudyDocument10 paginiInclusive Education Assignment 2 Case Studyapi-357570712Încă nu există evaluări
- Troy Ecological Congruence AssessmentDocument2 paginiTroy Ecological Congruence Assessmentapi-317339017100% (1)
- Teachers Attitudes Toward The Inclusion of Students With AutismDocument24 paginiTeachers Attitudes Toward The Inclusion of Students With Autismbig fourÎncă nu există evaluări
- Examining Student Behavior: Determining Intervention Through Deeper UnderstandingDocument17 paginiExamining Student Behavior: Determining Intervention Through Deeper Understandinggryphon688Încă nu există evaluări
- 4 3 1 Manage Challenging BehaviourDocument6 pagini4 3 1 Manage Challenging Behaviourapi-322000186Încă nu există evaluări
- Tier II Behavior Intervention Descriptions2Document13 paginiTier II Behavior Intervention Descriptions2api-233605048Încă nu există evaluări
- Classroom ManagementDocument17 paginiClassroom ManagementJuravle PetrutaÎncă nu există evaluări
- Stakeholder ChartDocument7 paginiStakeholder Chartapi-368273177100% (1)
- Ed5503 Final Project - Classroom ManagementDocument25 paginiEd5503 Final Project - Classroom Managementapi-437407548Încă nu există evaluări
- Vineland-Ii Presentation - Monique and Pat - Final VersionDocument22 paginiVineland-Ii Presentation - Monique and Pat - Final Versionapi-163017967Încă nu există evaluări
- Empowering Learnsers Through Self-RegulationDocument50 paginiEmpowering Learnsers Through Self-RegulationCarlo MagnoÎncă nu există evaluări
- Inclusive Education Assessment TwoDocument9 paginiInclusive Education Assessment Twoapi-464316796Încă nu există evaluări
- Cognitive FlexibilityDocument14 paginiCognitive Flexibilitydavidarbelo35100% (1)
- Man Jin 110158709-Workbook For Educ 5152Document5 paginiMan Jin 110158709-Workbook For Educ 5152api-351195320Încă nu există evaluări
- A Guide For Monitoring Child Development in Low - and Middle-Income CountriesDocument11 paginiA Guide For Monitoring Child Development in Low - and Middle-Income Countriesanisetiyowati14230% (1)
- Critical Thinking Final TermDocument54 paginiCritical Thinking Final TermM.Basit RahimÎncă nu există evaluări
- Actividad Entregable 2 - RoutinesDocument3 paginiActividad Entregable 2 - RoutinesAnggie ApoloÎncă nu există evaluări
- Pulpitis ReversiibleDocument7 paginiPulpitis ReversiibleAlsilaÎncă nu există evaluări
- Lesson Plan Songs and PoetryDocument13 paginiLesson Plan Songs and PoetryDeena ChandramohanÎncă nu există evaluări
- Cursos de Italiano PDFDocument16 paginiCursos de Italiano PDFmagaly125Încă nu există evaluări
- CV Dr. RiaDocument5 paginiCV Dr. RiaidaÎncă nu există evaluări
- 20 Points RubricsDocument1 pagină20 Points RubricsJerome Formalejo,Încă nu există evaluări
- Rubrics For Speaking CompetenceDocument1 paginăRubrics For Speaking CompetenceAMELYN DACULAÎncă nu există evaluări
- SOULFUL JAPA - Bliss Unlimited by Japa YagnaDocument28 paginiSOULFUL JAPA - Bliss Unlimited by Japa Yagnabalaganesh spk100% (1)
- Final Assessment PaperDocument11 paginiFinal Assessment PaperKevlyn HolmesÎncă nu există evaluări
- Bachelor of Science in Forestry: Quirino State University College of Agriculture, Forestry and EngineeringDocument12 paginiBachelor of Science in Forestry: Quirino State University College of Agriculture, Forestry and EngineeringJumreih Cacal100% (2)
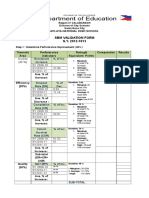
- SBM VAlidation FormDocument2 paginiSBM VAlidation FormamerizaÎncă nu există evaluări
- Public Storm Warning Signal (PSWS)Document5 paginiPublic Storm Warning Signal (PSWS)Jeric Rey AuditorÎncă nu există evaluări
- Strategic Management - Module 5 - Strategic Human Resource ManagementDocument4 paginiStrategic Management - Module 5 - Strategic Human Resource ManagementEva Katrina R. LopezÎncă nu există evaluări
- 2012 Introducing Health and Well-BeingDocument24 pagini2012 Introducing Health and Well-BeingvosoÎncă nu există evaluări
- Understanding College Students With Physical DisabilitiesDocument234 paginiUnderstanding College Students With Physical Disabilitieshana fentaÎncă nu există evaluări
- Practical Research 2 Chapter 1 Group11 Almost DoneDocument18 paginiPractical Research 2 Chapter 1 Group11 Almost DoneGin Ramos100% (1)
- Single Sex EducationDocument7 paginiSingle Sex EducationBreAnna SmithÎncă nu există evaluări
- Miss Bhagyashri Patil SIP ReportDocument71 paginiMiss Bhagyashri Patil SIP ReportDr. Sanket CharkhaÎncă nu există evaluări
- Features of 21st Century HRD and Training ProgramsDocument9 paginiFeatures of 21st Century HRD and Training Programstvglacaba1213100% (1)
- Philosophical Foundation of Education: PhilosophyDocument8 paginiPhilosophical Foundation of Education: PhilosophyKhadija Ali KhanÎncă nu există evaluări
- Comparative Study of English and ArabicDocument16 paginiComparative Study of English and ArabicHamid AlhajjajÎncă nu există evaluări
- The Writing Block: Cheryl M. SigmonDocument4 paginiThe Writing Block: Cheryl M. Sigmoneva.bensonÎncă nu există evaluări
- 5 Research Backed Study TechniquesDocument4 pagini5 Research Backed Study TechniquesUtpreksh PatbhajeÎncă nu există evaluări
- Press Release Brainly in The PhilippinesDocument1 paginăPress Release Brainly in The PhilippinesGiancarlo Muñoz ViterboÎncă nu există evaluări
- Translating A Competency Standard Into A Competency-Based CurriculumDocument11 paginiTranslating A Competency Standard Into A Competency-Based Curriculumxycor madlaÎncă nu există evaluări
- Orientation Guide - 12 Week YearDocument4 paginiOrientation Guide - 12 Week YearSachin Manjalekar89% (9)
- Aa-Matrix Company ProfileDocument23 paginiAa-Matrix Company ProfileBilly Joe BreakfastÎncă nu există evaluări
- Classification Epidemiological Studies PDFDocument17 paginiClassification Epidemiological Studies PDFAnonymous goIn6wA3KÎncă nu există evaluări
- Question Aware Vision Transformer For Multimodal ReasoningDocument15 paginiQuestion Aware Vision Transformer For Multimodal ReasoningOnlyBy MyselfÎncă nu există evaluări
- Propst ReportDocument5 paginiPropst ReportJosh Bean0% (1)