S-ar putea să vă placă și
- Bone Tumors2006Document89 paginiBone Tumors2006api-19916399Încă nu există evaluări
- Tumor Tulang Jinak: Anisah Mahmudah C014172125Document18 paginiTumor Tulang Jinak: Anisah Mahmudah C014172125Williamtatokieesz Tembokrumahampebenjol-benjolÎncă nu există evaluări
- Benign Bone Tumours Lecture - PpsDocument11 paginiBenign Bone Tumours Lecture - Ppsnickmirad2Încă nu există evaluări
- Review of Musculoskeletal TumorsDocument63 paginiReview of Musculoskeletal TumorsDanur AdiÎncă nu există evaluări
- General Information: Signs/SymptomsDocument17 paginiGeneral Information: Signs/SymptomsColesniuc CostiÎncă nu există evaluări
- BenignOsseousTumorsofBoneOsteoblastomaandOsteoid OsteDocument203 paginiBenignOsseousTumorsofBoneOsteoblastomaandOsteoid OstechikkisaurusÎncă nu există evaluări
- Bone InflammationDocument9 paginiBone InflammationBarettÎncă nu există evaluări
- Bone Tumor & Tumor-Like Lesions: By: Dr. Manal NageebDocument56 paginiBone Tumor & Tumor-Like Lesions: By: Dr. Manal NageebSonny WijanarkoÎncă nu există evaluări
- Delayed Union 0 Nonunion - Management PrincipleDocument50 paginiDelayed Union 0 Nonunion - Management PrincipleBimnilson SinghÎncă nu există evaluări
- Bone Tumors LectureDocument16 paginiBone Tumors LecturePrecious PipitÎncă nu există evaluări
- Tumor Unknown Conference ABC Case ReportsDocument46 paginiTumor Unknown Conference ABC Case ReportsAliyah Tofani PawelloiÎncă nu există evaluări
- X-Ray: Most Useful of All ImagingDocument33 paginiX-Ray: Most Useful of All ImagingDinesh VeraÎncă nu există evaluări
- Characteristics and Types of Benign Bone TumoursDocument11 paginiCharacteristics and Types of Benign Bone Tumourskyliever100% (1)
- Bone and Joint TumoursDocument49 paginiBone and Joint TumoursMahmoud Abu Al Amrain100% (1)
- Osteo Sarko Ma 1Document10 paginiOsteo Sarko Ma 1merizÎncă nu există evaluări
- Curs 9 Imagistica MSKDocument62 paginiCurs 9 Imagistica MSKn bÎncă nu există evaluări
- Bone and Joint Neoplasm or TumorDocument49 paginiBone and Joint Neoplasm or Tumorendah rahmadaniÎncă nu există evaluări
- Lecture 3 MuskDocument8 paginiLecture 3 MuskElgilani zaherÎncă nu există evaluări
- Tumors of MusculoskeletalDocument7 paginiTumors of MusculoskeletalodiliajessicanpviaÎncă nu există evaluări
- Benign Bone TumoursDocument13 paginiBenign Bone TumoursAnisah MahmudahÎncă nu există evaluări
- Neoplasm of Musculo SkeletalDocument70 paginiNeoplasm of Musculo SkeletalRiyan ArdiansyahÎncă nu există evaluări
- Imaging Manifestations of The Skeletal SystemDocument89 paginiImaging Manifestations of The Skeletal SystemGenki Anime GirlÎncă nu există evaluări
- Osteoarthritis & Rheumatoid ArthritisDocument60 paginiOsteoarthritis & Rheumatoid ArthritisSaya MenangÎncă nu există evaluări
- JCM 11 00699Document20 paginiJCM 11 00699OstazÎncă nu există evaluări
- Osteoid OsteomaDocument6 paginiOsteoid OsteomadrkaushikduttaÎncă nu există evaluări
- Classification and Imaging Features of Primary Bone TumorsDocument5 paginiClassification and Imaging Features of Primary Bone TumorsnmahpbooksÎncă nu există evaluări
- Xray of Bones in OsteomyelitisDocument35 paginiXray of Bones in OsteomyelitisBukola AjokeÎncă nu există evaluări
- Bone TumorsDocument58 paginiBone Tumorsdrqazi777Încă nu există evaluări
- Bone Tumours: - Jeffrey Pradeep RajDocument42 paginiBone Tumours: - Jeffrey Pradeep RajjeffreyprajÎncă nu există evaluări
- Diagnosis of Bone Tumours: 1. Age of Patient 2. Location of Tumour 3. Radiological Appearance 4. Histological FeaturesDocument69 paginiDiagnosis of Bone Tumours: 1. Age of Patient 2. Location of Tumour 3. Radiological Appearance 4. Histological Featuresyurie_ameliaÎncă nu există evaluări
- Skeletal Radiology Interpretation GuideDocument89 paginiSkeletal Radiology Interpretation GuideRivani KurniawanÎncă nu există evaluări
- PATH - Bony Tumours (6p)Document6 paginiPATH - Bony Tumours (6p)andreeaÎncă nu există evaluări
- 08 Bone TumorsDocument94 pagini08 Bone TumorsSara FoudaÎncă nu există evaluări
- Foot and Ankle Tumor Radiographic FeaturesDocument9 paginiFoot and Ankle Tumor Radiographic FeaturesShazeb RizviÎncă nu există evaluări
- Non-Odontogenic Tumor (Lecture)Document64 paginiNon-Odontogenic Tumor (Lecture)shabeelpn86% (7)
- Benign Bone Tumors and Reactive LesionsDocument91 paginiBenign Bone Tumors and Reactive LesionsYohannisNigusuÎncă nu există evaluări
- Neoplasm of Musculoskeletal Tissue: A GuideDocument48 paginiNeoplasm of Musculoskeletal Tissue: A Guidehello from the other sideÎncă nu există evaluări
- Malignant Bone PathologyDocument25 paginiMalignant Bone PathologySaski salsaaÎncă nu există evaluări
- Booooooone Tumors REFERATDocument47 paginiBooooooone Tumors REFERATNurlaila IshaqÎncă nu există evaluări
- BoneDocument68 paginiBonedr_asaleh100% (2)
- Bone TumoursDocument22 paginiBone TumoursAnis Ahmed BelkhodjaÎncă nu există evaluări
- Case Reflection of OsteochondromaDocument21 paginiCase Reflection of OsteochondromaBenny Yohanis GaeÎncă nu există evaluări
- Orthopedic Tumors and OsteoarthritisDocument6 paginiOrthopedic Tumors and OsteoarthritisSai Snigdha MohantyÎncă nu există evaluări
- Benign Non Odontogenic Lesions - 6Document97 paginiBenign Non Odontogenic Lesions - 6Thaer ZabenÎncă nu există evaluări
- BoneDocument34 paginiBoneKushagraSharmaÎncă nu există evaluări
- Radiologic Imaging of MuskuloskeletalDocument42 paginiRadiologic Imaging of MuskuloskeletalfennyhasanahÎncă nu există evaluări
- Temporo Mandibular Joint Disorder Oral SurgeryDocument59 paginiTemporo Mandibular Joint Disorder Oral SurgeryFourthMolar.comÎncă nu există evaluări
- Tumor Flash Cards - Osteochondroma and Multiple Hereditary ExostosisDocument23 paginiTumor Flash Cards - Osteochondroma and Multiple Hereditary Exostosislaxge54Încă nu există evaluări
- Benign Bone TumorDocument28 paginiBenign Bone Tumorمحمد خالد البردومي المريسيÎncă nu există evaluări
- Bone tm3Document57 paginiBone tm3ZakiyahulfahdwÎncă nu există evaluări
- Bone Tumor Diagnosis and ManagementDocument23 paginiBone Tumor Diagnosis and ManagementRiyaduÎncă nu există evaluări
- Bone and Soft Tissue TumoursDocument9 paginiBone and Soft Tissue TumoursSurgicalgownÎncă nu există evaluări
- Severe TMJ OA PDFDocument6 paginiSevere TMJ OA PDFHồ TiênÎncă nu există evaluări
- Malignant Bone PathologyDocument25 paginiMalignant Bone PathologySaski salsaaÎncă nu există evaluări
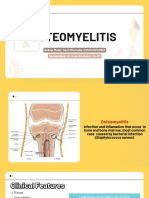
- OsteomyelitisDocument15 paginiOsteomyelitis2018B-04Desti RhomaliaÎncă nu există evaluări
- Bone TumorDocument36 paginiBone TumorMoch NizamÎncă nu există evaluări
- Seminar W4 - Bone & Soft Tissue TumoursDocument123 paginiSeminar W4 - Bone & Soft Tissue TumoursUN EPÎncă nu există evaluări
- Your Family Doctor Arthritis: Rheumatoid Arthritis / Osteo-arthritis / Gout / OsteoporosisDe la EverandYour Family Doctor Arthritis: Rheumatoid Arthritis / Osteo-arthritis / Gout / OsteoporosisEvaluare: 1 din 5 stele1/5 (1)
- Carpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsDe la EverandCarpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsEvaluare: 5 din 5 stele5/5 (1)
- Inlay OnlayDocument21 paginiInlay OnlaySawsan Z. Jwaied100% (1)
- Radio Questions Solved by Sawsan JwaiedDocument21 paginiRadio Questions Solved by Sawsan JwaiedSawsan Z. JwaiedÎncă nu există evaluări
- Torus ManDocument3 paginiTorus ManSawsan Z. JwaiedÎncă nu există evaluări
- AbfoDocument3 paginiAbfoSawsan Z. JwaiedÎncă nu există evaluări
- December, 11th 2013: What Is An Emergency?Document11 paginiDecember, 11th 2013: What Is An Emergency?Sawsan Z. JwaiedÎncă nu există evaluări
- AbfDocument5 paginiAbfSawsan Z. JwaiedÎncă nu există evaluări
- Exostosis PDFDocument3 paginiExostosis PDFSawsan Z. JwaiedÎncă nu există evaluări
- OM Lec1 HandoutDocument2 paginiOM Lec1 HandoutSawsan Z. JwaiedÎncă nu există evaluări
- Cons 10Document11 paginiCons 10Sawsan Z. JwaiedÎncă nu există evaluări
- Osteo SclerosisDocument3 paginiOsteo SclerosisSawsan Z. JwaiedÎncă nu există evaluări
- AotDocument3 paginiAotSawsan Z. JwaiedÎncă nu există evaluări
- Torus PalatDocument3 paginiTorus PalatSawsan Z. JwaiedÎncă nu există evaluări
- CeotDocument3 paginiCeotSawsan Z. JwaiedÎncă nu există evaluări
- AbDocument5 paginiAbSawsan Z. JwaiedÎncă nu există evaluări
- MyxomaDocument3 paginiMyxomaSawsan Z. JwaiedÎncă nu există evaluări
- CofDocument3 paginiCofSawsan Z. JwaiedÎncă nu există evaluări
- Odon TomDocument4 paginiOdon TomSawsan Z. JwaiedÎncă nu există evaluări
- CBDocument3 paginiCBSawsan Z. JwaiedÎncă nu există evaluări
- HemangiomaDocument3 paginiHemangiomaSawsan Z. JwaiedÎncă nu există evaluări
- DFDocument3 paginiDFSawsan Z. JwaiedÎncă nu există evaluări
- Osteo Blast OmaDocument3 paginiOsteo Blast OmaSawsan Z. JwaiedÎncă nu există evaluări
- Osteo MaDocument3 paginiOsteo MaSawsan Z. JwaiedÎncă nu există evaluări
- Composite Resin RestorationDocument9 paginiComposite Resin RestorationSawsan Z. JwaiedÎncă nu există evaluări
- Schwann OmaDocument4 paginiSchwann OmaSawsan Z. JwaiedÎncă nu există evaluări
- Nerve Sheath TumorDocument4 paginiNerve Sheath TumorSawsan Z. JwaiedÎncă nu există evaluări
- Cont Script3Document9 paginiCont Script3Sawsan Z. JwaiedÎncă nu există evaluări
- NFDocument5 paginiNFSawsan Z. JwaiedÎncă nu există evaluări
- Periodontal Instrumentation: Non Surgical TreatmentDocument15 paginiPeriodontal Instrumentation: Non Surgical TreatmentSawsan Z. JwaiedÎncă nu există evaluări
- Summery of TechniquesDocument1 paginăSummery of TechniquesSawsan Z. JwaiedÎncă nu există evaluări
- Biodata: PARGANAS, KOLKATA-700102, West BengalDocument3 paginiBiodata: PARGANAS, KOLKATA-700102, West BengalTina lovelyÎncă nu există evaluări
- Cardiology OSCEDocument35 paginiCardiology OSCEvigneshmmc02Încă nu există evaluări
- Giant Sialolithiasis - Diagnosis and Management. Case Reports.Document3 paginiGiant Sialolithiasis - Diagnosis and Management. Case Reports.Mihaela DandaraÎncă nu există evaluări
- GIMMI NeurosurgeryDocument222 paginiGIMMI NeurosurgerysigmakarsaÎncă nu există evaluări
- Non Opioid DrugsDocument43 paginiNon Opioid DrugsSlamet KatibÎncă nu există evaluări
- VEP TeachingGuide PDFDocument162 paginiVEP TeachingGuide PDFAdriana LopezÎncă nu există evaluări
- Drug Study: Cavite State University (Cvsu)Document2 paginiDrug Study: Cavite State University (Cvsu)Angelica Cassandra VillenaÎncă nu există evaluări
- St. Victoria Hospital Nursing Service Ward DeptDocument50 paginiSt. Victoria Hospital Nursing Service Ward DeptPat MagpaliÎncă nu există evaluări
- Premature Rupture of The MembraneDocument27 paginiPremature Rupture of The MembranezizsatriaÎncă nu există evaluări
- MCQs For The FRCS (Urol) and Postgraduate Urology ExaminationsDocument241 paginiMCQs For The FRCS (Urol) and Postgraduate Urology ExaminationsHaryo Prakoso Adhi PÎncă nu există evaluări
- Virtual Pig Dissection Worksheet 06-07 2Document6 paginiVirtual Pig Dissection Worksheet 06-07 2api-255054890Încă nu există evaluări
- Awesome Birthe BookDocument278 paginiAwesome Birthe BookOlga SilvaÎncă nu există evaluări
- Maternity NursingDocument24 paginiMaternity NursingJen Arcillas Tuble - Iledan100% (1)
- II. Subdivisions of PathologyDocument2 paginiII. Subdivisions of PathologySiegÎncă nu există evaluări
- Neonatal JaundiceDocument4 paginiNeonatal JaundiceChristian Eduard de DiosÎncă nu există evaluări
- Reproductive Toxicity Testing: What and Why?: TOPRA Annual Veterinary SymposiumDocument51 paginiReproductive Toxicity Testing: What and Why?: TOPRA Annual Veterinary Symposiuml3ly0709Încă nu există evaluări
- ASHA LeafletDocument4 paginiASHA LeafletDINESHÎncă nu există evaluări
- Kel 3 A Midwifery Model of Care ForDocument13 paginiKel 3 A Midwifery Model of Care ForWawa KurniaÎncă nu există evaluări
- Lower Extremity Stretching For Endurance RunnersDocument4 paginiLower Extremity Stretching For Endurance RunnersCristian YanezÎncă nu există evaluări
- Antenatal Assessment of Foetal Wellbeing.Document30 paginiAntenatal Assessment of Foetal Wellbeing.Kavya S MohanÎncă nu există evaluări
- TSBDocument4 paginiTSBpfpkiÎncă nu există evaluări
- GC Fuji Vii: Clinical ApplicationsDocument5 paginiGC Fuji Vii: Clinical ApplicationsLisna K. RezkyÎncă nu există evaluări
- MM Ob Gyn Catalog WebDocument100 paginiMM Ob Gyn Catalog Webthumper2madÎncă nu există evaluări
- MTurbo System SpecificationDocument2 paginiMTurbo System SpecificationSerban MihaelaÎncă nu există evaluări
- Al Manar Hospital Mohammadpur Doctor List & ContactDocument1 paginăAl Manar Hospital Mohammadpur Doctor List & Contactrubayat112015Încă nu există evaluări
- Nursing Care Plan: Interaction Immediate Cause Goal: Effectivenes SDocument6 paginiNursing Care Plan: Interaction Immediate Cause Goal: Effectivenes SCatherine Kaye Marquez RoxasÎncă nu există evaluări
- Medical Ethics Dissertation TopicsDocument8 paginiMedical Ethics Dissertation TopicsThesisPaperHelpCanada100% (1)
- CPT PDFDocument43 paginiCPT PDFEbony Crawford100% (1)
- Uog15821 Online PDFDocument17 paginiUog15821 Online PDFernestosandÎncă nu există evaluări
- Chalian Maxillofacial Prosthetics PDFDocument472 paginiChalian Maxillofacial Prosthetics PDFVyoma100% (13)