S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Einstein 1937Document12 paginiEinstein 1937JonathanHdzÎncă nu există evaluări
- Eklavya Central Shool, Saharsa: Holiday HomeworkDocument3 paginiEklavya Central Shool, Saharsa: Holiday HomeworkChitrakumariÎncă nu există evaluări
- OOPM Theory QuestionsDocument7 paginiOOPM Theory Questionssheenam_bhatiaÎncă nu există evaluări
- GPS Constellation Toolbox Manual-Version70Document131 paginiGPS Constellation Toolbox Manual-Version70bdkim90Încă nu există evaluări
- Tutorial Letter 001/3/2021: Complex AnalysisDocument19 paginiTutorial Letter 001/3/2021: Complex AnalysisKyle MaharajÎncă nu există evaluări
- Package Survival': R Topics DocumentedDocument185 paginiPackage Survival': R Topics DocumentedFlorencia FirenzeÎncă nu există evaluări
- E & P Cycle in Petroleum Industry: A Question of Risk and UncertaintyDocument38 paginiE & P Cycle in Petroleum Industry: A Question of Risk and UncertaintyAdvait DeshmukhÎncă nu există evaluări
- Chapter 2: Basic Concepts of Probability Theory: 2.1 Specifying Random ExperimentsDocument6 paginiChapter 2: Basic Concepts of Probability Theory: 2.1 Specifying Random ExperimentsSonam AlviÎncă nu există evaluări
- HW 1 SolutionsDocument3 paginiHW 1 Solutionszainab alshatterÎncă nu există evaluări
- 01otr 02ourDocument53 pagini01otr 02ourKeerthana KÎncă nu există evaluări
- Numerical Simulations of A Scramjet Isolator Using RANS and LES ApproachesDocument9 paginiNumerical Simulations of A Scramjet Isolator Using RANS and LES ApproachesHoàng DavidÎncă nu există evaluări
- L As Level Physics A 2821 01 January 2008 Question Paper Old g481Document16 paginiL As Level Physics A 2821 01 January 2008 Question Paper Old g481dasha962Încă nu există evaluări
- Lec 10Document4 paginiLec 10RKD CinemaÎncă nu există evaluări
- Hydrocyclones For Particle Size SeparationDocument7 paginiHydrocyclones For Particle Size SeparationJean DejardinÎncă nu există evaluări
- House Price Estimates Based On Machine Learning AlgorithmDocument5 paginiHouse Price Estimates Based On Machine Learning AlgorithmEditor IJTSRDÎncă nu există evaluări
- 33 As Statistics Unit 5 TestDocument2 pagini33 As Statistics Unit 5 TestThomas BeerÎncă nu există evaluări
- 9709 w10 QP 61Document4 pagini9709 w10 QP 61Sherman TanÎncă nu există evaluări
- Notes On Algbra G ChrystalDocument31 paginiNotes On Algbra G ChrystalstreetbaÎncă nu există evaluări
- The Mechanism of Activated Digusion Through Silica GlassDocument9 paginiThe Mechanism of Activated Digusion Through Silica GlassElenaÎncă nu există evaluări
- Example: Triangle On A Face IconDocument26 paginiExample: Triangle On A Face IconGinalyn QuimsonÎncă nu există evaluări
- EE5143 Tutorial1Document5 paginiEE5143 Tutorial1Sayan Rudra PalÎncă nu există evaluări
- MECH60561 2022 23 Pressure Vessel ExerciseDocument3 paginiMECH60561 2022 23 Pressure Vessel ExerciseAli JabranÎncă nu există evaluări
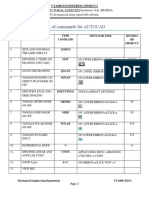
- List of Commands For Autocad: Cad Lab Tutorial Exercises Instructor: S.K. Sharma To Be Practiced Using Autocad SoftwareDocument15 paginiList of Commands For Autocad: Cad Lab Tutorial Exercises Instructor: S.K. Sharma To Be Practiced Using Autocad SoftwareShakeelÎncă nu există evaluări
- Programmable Logic ControllersDocument31 paginiProgrammable Logic Controllersgpz10100% (15)
- Density 1 QPDocument11 paginiDensity 1 QPHammad Ahmed50% (2)
- Biaxial Bending (Beams in Both Axis) : Ce 514 - Steel DesignDocument6 paginiBiaxial Bending (Beams in Both Axis) : Ce 514 - Steel DesignFrederick Perez IIÎncă nu există evaluări
- Physics Lab Report Newton2.docx 2Document18 paginiPhysics Lab Report Newton2.docx 2Omar MustafaÎncă nu există evaluări
- Adaptive Control Design and AnalysisDocument45 paginiAdaptive Control Design and Analysishind90Încă nu există evaluări
- ECON301 Handout 04 1415 02Document17 paginiECON301 Handout 04 1415 02ffef fefffÎncă nu există evaluări
- Discuss The Concept of Semantics and Elaborate NameDocument4 paginiDiscuss The Concept of Semantics and Elaborate NameAnonymous R99uDjYÎncă nu există evaluări