S-ar putea să vă placă și
- Megaloblastic and Other Macrocytic Anaemia: Dr. Nilukshi Perera Consultant HaematologistDocument58 paginiMegaloblastic and Other Macrocytic Anaemia: Dr. Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhiteÎncă nu există evaluări
- Anemia: Iron Deficiency Vit B12 Folate DeficiencyDocument33 paginiAnemia: Iron Deficiency Vit B12 Folate DeficiencymoosaicqÎncă nu există evaluări
- Hematopoiesis Anemia: Composition of The BloodDocument16 paginiHematopoiesis Anemia: Composition of The BloodOcha24 TupamahuÎncă nu există evaluări
- Basic Lab InvestigationsDocument121 paginiBasic Lab InvestigationsTheop Ayodele100% (1)
- Case 21Document45 paginiCase 21Mark GironÎncă nu există evaluări
- Megaloblastic AnemiaDocument5 paginiMegaloblastic AnemiaNTA UGC-NETÎncă nu există evaluări
- 209-Hematology Review - Case StudiesDocument129 pagini209-Hematology Review - Case StudiesKhalid Khalidi100% (2)
- Class 3: Anemia Outline I. Anemia OverviewDocument4 paginiClass 3: Anemia Outline I. Anemia OverviewTonyÎncă nu există evaluări
- Red Cell Disorders: Excellent in Quality, Competitiveness, and CareDocument43 paginiRed Cell Disorders: Excellent in Quality, Competitiveness, and CareDeriven Teweng0% (1)
- Heamtology Reviewer (Midterm)Document15 paginiHeamtology Reviewer (Midterm)Johney DoeÎncă nu există evaluări
- What Is Anemia, How Do You Diagnose Anemia, and How Are The Different Anemias Classified?Document60 paginiWhat Is Anemia, How Do You Diagnose Anemia, and How Are The Different Anemias Classified?Priyanka MhÎncă nu există evaluări
- Pernicious Anemia: BSMT 3D Group 1 Paniza, Erika Joy Villanueva, Andrewarnold Yandan, CharisDocument53 paginiPernicious Anemia: BSMT 3D Group 1 Paniza, Erika Joy Villanueva, Andrewarnold Yandan, CharisAndrew Arnold David VillanuevaÎncă nu există evaluări
- HolotranscobalaminDocument43 paginiHolotranscobalaminAndrés Menéndez Rojas100% (1)
- An Approach To Anemia 4-3-03: - Bob Richard - Faculty - Washington.edu/rrichard Connect To Talks For HandoutDocument77 paginiAn Approach To Anemia 4-3-03: - Bob Richard - Faculty - Washington.edu/rrichard Connect To Talks For HandoutYen-Jen SungÎncă nu există evaluări
- Interpreting The CBC - When To ReferDocument44 paginiInterpreting The CBC - When To ReferKannan KannanÎncă nu există evaluări
- An Approach To Anemia 4-3-03: - Bob Richard - Faculty - Washington.edu/rrichard Connect To Talks For HandoutDocument77 paginiAn Approach To Anemia 4-3-03: - Bob Richard - Faculty - Washington.edu/rrichard Connect To Talks For HandoutrhondreaÎncă nu există evaluări
- Anaemia: What Is Anemia?Document21 paginiAnaemia: What Is Anemia?Rashed ShatnawiÎncă nu există evaluări
- Anemia Is A Laboratory Diagnosis: Men WomenDocument21 paginiAnemia Is A Laboratory Diagnosis: Men WomenOmaraye JoshuaÎncă nu există evaluări
- 13.2 AnemiaDocument75 pagini13.2 AnemiaMohammad AlrefaiÎncă nu există evaluări
- Evaluation of The Anemic PatientDocument44 paginiEvaluation of The Anemic PatientShobana KmÎncă nu există evaluări
- Macrocytic Anemias: Defective DNA SynthesisDocument17 paginiMacrocytic Anemias: Defective DNA SynthesispallavberiÎncă nu există evaluări
- Anemia OsamaDocument57 paginiAnemia Osamaosamafoud7710Încă nu există evaluări
- Approuch Anemia On Laboratory Based: Hematology 2011Document31 paginiApprouch Anemia On Laboratory Based: Hematology 2011VincentiusÎncă nu există evaluări
- Blood Disorder in PregnancyDocument43 paginiBlood Disorder in PregnancyNadhrah zulkifliÎncă nu există evaluări
- K - 13 Anemia Defisiensi Besi (Ilmu Kesehatan Anak)Document68 paginiK - 13 Anemia Defisiensi Besi (Ilmu Kesehatan Anak)RabiahIrfahÎncă nu există evaluări
- Anemia OsamaDocument57 paginiAnemia Osamaosamafoud7710Încă nu există evaluări
- Nutritional AnemiaDocument53 paginiNutritional AnemiaANUREET KAURÎncă nu există evaluări
- Blok 5 Antianaemic DrugsDocument26 paginiBlok 5 Antianaemic DrugsPutri HusnanÎncă nu există evaluări
- Approach To Pale ChildDocument37 paginiApproach To Pale ChildsangheetaÎncă nu există evaluări
- RBC DISORDERS StudentsDocument84 paginiRBC DISORDERS Studentskimberly abianÎncă nu există evaluări
- Haematinics & ErythropoietinDocument30 paginiHaematinics & ErythropoietinManikanta GupthaÎncă nu există evaluări
- Macrocytic AnemiasDocument28 paginiMacrocytic AnemiasDeepankar SrigyanÎncă nu există evaluări
- Abnormal CBC - PresentationDocument23 paginiAbnormal CBC - PresentationMateen ShukriÎncă nu există evaluări
- Megaloblastic AneamiaDocument74 paginiMegaloblastic AneamiaPhysiology by Dr RaghuveerÎncă nu există evaluări
- Quiz YourselfDocument154 paginiQuiz YourselfKandykane05100% (1)
- AnemiaDocument93 paginiAnemiaShalini ChanduÎncă nu există evaluări
- PejowebApproach To Anemia by Dr. Joel Solorzani RomeroDocument57 paginiPejowebApproach To Anemia by Dr. Joel Solorzani RomeroAshraf FaragÎncă nu există evaluări
- Management of Patient With AnemiaDocument58 paginiManagement of Patient With AnemiaDoaa HussainÎncă nu există evaluări
- Anemia EngDocument49 paginiAnemia EngingritfuryÎncă nu există evaluări
- Case Study: Ellah Saab, Jamilah Latip, Jenny Bacomo, Gaylle Gonzaga, Martha Suyao, Jezza Leigh, Gwen LagnasonDocument33 paginiCase Study: Ellah Saab, Jamilah Latip, Jenny Bacomo, Gaylle Gonzaga, Martha Suyao, Jezza Leigh, Gwen LagnasonEllah SaabÎncă nu există evaluări
- Approuch Anemia PBLDocument31 paginiApprouch Anemia PBLAndy XiaoÎncă nu există evaluări
- Red Cell DisorderDocument43 paginiRed Cell DisorderYuliusDenisChrismaajiÎncă nu există evaluări
- Megaloblastic AnemiaDocument26 paginiMegaloblastic AnemiaAbdifatah Abdiwali mohamedÎncă nu există evaluări
- ABP3 IntoxmetalespesadosDocument18 paginiABP3 IntoxmetalespesadosFernandoLuyoÎncă nu există evaluări
- RBC DisordersDocument49 paginiRBC DisordersGeraldine AgpesÎncă nu există evaluări
- Anaemi A: Joshi Abhishek Ashvinbhai F.Y.P.B.B.Sc - Nursing Govt - College of Nursing JamnagarDocument82 paginiAnaemi A: Joshi Abhishek Ashvinbhai F.Y.P.B.B.Sc - Nursing Govt - College of Nursing JamnagarReshu ThakuriÎncă nu există evaluări
- AMK Diseases p2Document292 paginiAMK Diseases p2hanif ahmadÎncă nu există evaluări
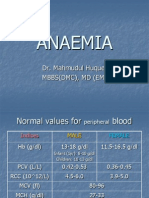
- Anaemia: Dr. Mahmudul Huque. Mbbs (DMC), MD (Em)Document32 paginiAnaemia: Dr. Mahmudul Huque. Mbbs (DMC), MD (Em)Junayed Safar MahmudÎncă nu există evaluări
- Anemia SDocument125 paginiAnemia SamirhsheikhiÎncă nu există evaluări
- Anemia and Its Classification by DR Bashir Ahmed Dar A Sopore Kashmir 1228039135310976 9Document30 paginiAnemia and Its Classification by DR Bashir Ahmed Dar A Sopore Kashmir 1228039135310976 9hercolaniumÎncă nu există evaluări
- AneamiaDocument27 paginiAneamiaNatif BoteÎncă nu există evaluări
- Haematology II Past Papers 3rd YearDocument11 paginiHaematology II Past Papers 3rd YearSyed Muhammad HameemÎncă nu există evaluări
- Heamatological Disorder: Disorder Related To Red Blood CellDocument12 paginiHeamatological Disorder: Disorder Related To Red Blood CellHelmiÎncă nu există evaluări
- Blood DisordersDocument10 paginiBlood DisordersJohn PaulÎncă nu există evaluări
- Approach To Pediatric AnemiaDocument18 paginiApproach To Pediatric AnemiaMade Oka HeryanaÎncă nu există evaluări
- Hematology Tests - G I SVDocument49 paginiHematology Tests - G I SVSV. Trần Hữu ThắngÎncă nu există evaluări
- Megaloblastic AnaemiaDocument11 paginiMegaloblastic AnaemiaJesmin_36Încă nu există evaluări
- AnemiaDocument32 paginiAnemiaJawad SaleemÎncă nu există evaluări
- Anemia in ChildrenDocument67 paginiAnemia in ChildrenAgung Maulana ArmstrongÎncă nu există evaluări
- MeningomyeloceleDocument42 paginiMeningomyeloceleSundaraBharathiÎncă nu există evaluări
- Kaplan Decision Tree and All Nurses NotesDocument103 paginiKaplan Decision Tree and All Nurses NotesTravel Junky100% (1)
- 10 Foods That Fight Cancer CellsDocument5 pagini10 Foods That Fight Cancer CellsNaushad AlamÎncă nu există evaluări
- VitaminesDocument76 paginiVitaminesFasika MeketeÎncă nu există evaluări
- Nutritional Deficiency For ClassDocument74 paginiNutritional Deficiency For ClassBelayneh TadesseÎncă nu există evaluări
- Manual of Clinical Nutrition2013Document458 paginiManual of Clinical Nutrition2013Jeffrey Wheeler100% (9)
- Babycare Before Birth, 2006Document146 paginiBabycare Before Birth, 2006Loredana Georgescu100% (7)
- Obstetric NursingDocument36 paginiObstetric NursingpauchanmnlÎncă nu există evaluări
- GayaHidup Feb 2012Document19 paginiGayaHidup Feb 2012Raynold Clare JohnÎncă nu există evaluări
- AnemiaDocument11 paginiAnemiadewiq_wahyuÎncă nu există evaluări
- Biochemistry Mnemonics PDFDocument16 paginiBiochemistry Mnemonics PDFfaraz50% (2)
- Biochemistry & Genetics Important Concepts Q&as DR Kumar Ponnusamy & Jegathambigai RN, Biochemistry & Genetics, International Medical University (IMU) / AIMST University School of Medicine, MalaysiaDocument60 paginiBiochemistry & Genetics Important Concepts Q&as DR Kumar Ponnusamy & Jegathambigai RN, Biochemistry & Genetics, International Medical University (IMU) / AIMST University School of Medicine, MalaysiaDr Kumar Ponnusamy100% (3)
- Water, Vitamins & MineralsDocument38 paginiWater, Vitamins & MineralsmalaitamanÎncă nu există evaluări
- Basic Need For GeriatricsDocument38 paginiBasic Need For GeriatricsMuhammad Yatsrib SemmeÎncă nu există evaluări
- Heamtology Reviewer (Midterm)Document15 paginiHeamtology Reviewer (Midterm)Johney DoeÎncă nu există evaluări
- Interaksi ObatDocument83 paginiInteraksi ObatGeronimouzt LoverzÎncă nu există evaluări
- Vitamins and Minerals: Nutrient (Vitamins) Needed For Key SourcesDocument4 paginiVitamins and Minerals: Nutrient (Vitamins) Needed For Key SourcesKevin Carl A. CorpuzÎncă nu există evaluări
- Douglas Ultra Preventive XDocument4 paginiDouglas Ultra Preventive XGary MollerÎncă nu există evaluări
- Espinosa, Kristine M. Bsn-IDocument5 paginiEspinosa, Kristine M. Bsn-ICamille EspinosaÎncă nu există evaluări
- Water Soluble VitaminsDocument33 paginiWater Soluble VitaminsRhomizal MazaliÎncă nu există evaluări
- Agents Used in AnemiasDocument26 paginiAgents Used in AnemiasHajrahPalembangan100% (1)
- Managing Disease and Avoiding Complications Through Diet Diversification - PPTX 31.10.14Document134 paginiManaging Disease and Avoiding Complications Through Diet Diversification - PPTX 31.10.14iqraÎncă nu există evaluări
- Children With Spina BifidaDocument14 paginiChildren With Spina Bifidafabsscribdworks100% (1)
- Health Benefits of SquashDocument9 paginiHealth Benefits of SquashBeth Bauzon100% (1)
- Reproductive Health Lesson PlanDocument103 paginiReproductive Health Lesson PlanJoe Marie A Mendoza100% (1)
- Nudietvitamins, Minerals & WaterDocument51 paginiNudietvitamins, Minerals & WaterDarlen RabanoÎncă nu există evaluări
- Gastrointestinal System and Nutrition Drug ChartsDocument3 paginiGastrointestinal System and Nutrition Drug ChartsNursingSchoolNotesÎncă nu există evaluări
- 7 Megaloblastic AnemiaDocument20 pagini7 Megaloblastic Anemiarajvikram87Încă nu există evaluări
- Nutrition Guideline PregnancyDocument27 paginiNutrition Guideline PregnancyMuhammad FauziÎncă nu există evaluări