Continuing Medical Education
Interpretation of liver enzyme tests
A rapid guide
Alan Fraser
Correspondence to: a.fraser@auckland .ac.nz
This guide (updated from an earlier version published in the NZFP in 20021) is intended to provide easily accessible information on appropriate investigation and likely diagnoses. First view Figure 1, then look at notes as indicated. For single enzyme elevations see Note 1. If multiple enzyme abnormalities refer to Question 1.
Alan Fraser is a Gastroenterologist and Associate Professor in Medicine at the University of Auckland. He is the author and webmaster for a patient information website called Gastro Info. This has comprehensive but easily readable information for all gastrointestinal and liver disease.
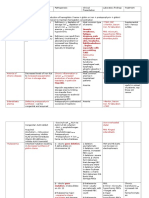
Figure 1. Elevated liver enzymes
ELEVATED LIVER ENZYMES (for single enzyme elevations see Note 1)
Hepatocellular ALT / AST
Cholestatic Alk phos / GGT
Acute
Chronic (>6/12)
Jaundice or pain
No pain and normal bilirubin Normal ultrasound
EBV, Hep A, B Alcohol, drugs (Note 2)
Hep B, C, fatty liver Iron overload, alcohol Drugs, autoimmune (Note 3)
Urgent ultrasound Specialist referral
Drugs, inflammation, malignancy Primary biliary cirrhosis, PSC (Note 5)
Check for evidence of cirrhosis Albumin, Prothrombin ratio Thrombocytopaenia (Note 4)
194
Volume 34 Number 3, June 2007
Continuing Medical Education
Note 1: Single enzyme elevation
GGT
Consider alcohol check for elevated MCV as further evidence. Heavy weekend drinking leads to elevation of 13x; peak at two to three days. Higher levels may take several weeks to resolve after abstinence from alcohol. Check drugs in particular phenytoin, carbamazepine, OC, rifampicin. Consider fatty liver risk factors are obesity, diabetes and elevated lipids. Ultrasound may confirm fatty liver by showing increased echogenicity (see also Note 3). The measurement of direct/indirect fraction (conjugated/unconjugated) is rarely useful in adult practice. Question 1. Is the pattern hepatocellular (mainly AST / ALT) OR cholestatic (mainly alkaline phosphatase and GGT) If mainly hepatocellular then refer to Question 2. If it is a mixture of both patterns, the predominant problem is usually obvious. Mild cholestasis is common with chronic hepatitis but the pattern is predominantly hepatocellular. In acute biliary obstruction a rise in AST/ALT may occur during the first two to three days (in addition to cholestatic picture) but returns to near normal if obstruction persists. Note that acute obstruction is usually associated with biliary-type pain. Question 2. Is there evidence of persistent elevation of AST/ALT over more than one to two months? More than six months of abnormal ALT/AST defines chronic hepatitis. In practical terms chronic hepatitis should be considered from the onset and becomes more likely if persistent abnormalities after one to two months. Many patients with newly discovered elevation of ALT/AST will prove to have chronic liver disease. If the initial level of ALT/AST is greater than 500IU then most likely to be acute hepatitis/liver injury. always asymptomatic. Hepatitis D only occurs in the presence of Hepatitis B infection). Consider drugs may also have rash, fever and eosinophilia (phenytoin, isoniazid, diclofenac, pirioxicam, allopurinol, azathioprine). Consider alcohol-induced liver disease. May cause hepatitis AST/ALT levels are relatively low for acute hepatitis (100300U/L). Also look for elevated GGT (100 300) but normal alkaline phosphatase, macrocytosis, AST greater than ALT (ratio >2.0 very suggestive), elevated WBC and fever if more severe hepatitis. Diagnosis of alcohol-related liver disease rests primarily on history and a high index of suspicion rather than pattern of liver test. Rarely auto-immune hepatitis can present as an acute illness. Even rarer Wilsons disease can be considered if <40 years check serum copper and ceruloplasmin.
Alkaline phosphatase
Elevation of alkaline phosphatase without elevation of GGT is very suggestive of bone disease e.g. recent fracture, Pagets disease. Normal elevation adolescents, 3rd trimester of pregnancy.
ALT
Can be mildly elevated with obesity and does not represent liver disease. Seems to relate directly to BMI (same is true for AST). In mild chronic hepatitis ALT may be elevated and the AST normal because of the higher sensitivity of ALT to hepatic inflammation.
Note 3: Tests for chronic hepatitis
Order relevant tests if ALT levels have been elevated for more than one to two months. In chronic hepatitis ALT usually only 1.53x upper limit of normal range. Request Hepatitis BsAg, Hepatitis C Ab (following by Hep C PCR if antibody positive), auto-antibodies (antinuclear antibody and smooth muscle antibody), serum ferritin and iron studies (serum Fe and TIBC). Commonest cause of raised ALT/ AST (usually associated with mild elevation of GGT) is fatty liver. If the fat deposition in the liver is associated with hepatic inflammation then this is called steatohepatitis. This occurs with excess alcohol intake but often is present in absence of alcohol (can be called non-alcoholic steatohepatits NASH). The risk factors for this condition are diabetes, elevated triglycerides (more important than cho-
AST
Consider recent muscle injury or bruising. May have acute rise of 23x after strenuous exercise. Check for haemolysis blood screen, haptoglobins, Coombs test. If persistent and no suggestion of liver disease, consider chronic muscle diseases, e.g. polymyositis measure creatinine kinase.
Note 2: Tests for acute hepatitis
Acute hepatitis is usually associated with symptoms of an acute illness. Commonest cause of acute elevation of ALT/AST in the community is infectious mononucleosis. Main tests for acute viral hepatitis are Hepatitis A IgM and Hepatitis BsAg and tests for EBV (50%) and CMV (<2%). (Hepatitis C does cause acute hepatitis but is almost
Bilirubin
Gilberts syndrome persistent but mild elevation of bilirubin but normal liver enzymes commonly elevated further with illness and fasting. Usually the levels are only up to 50umol/L (rarely up to 80umol/L).
Volume 34 Number 3, June 2007
195
Continuing Medical Education
lesterol), and obesity (waist circumference most predictive). Therefore should measure fasting glucose (sometimes GTT), HbA1c and fasting lipids. The fatty infiltration in the liver is detected by ultrasound of the liver in 6070% of cases. Raised ferritin may be due to hemochromatosis (see article on raised ferritin2) but also occurs with liver inflammation (common with fatty liver and excess alcohol consumption). Raised ferritin and normal iron saturation more likely to be fatty liver request liver ultrasound. If high iron saturation (>55%) order gene test for haemochromatosis (Cys282). Consider drugs can be any drug isoniazid, nitrofurantion, ketoconazole, NSAIDs. Consider also illicit drugs, anabolic steroids and herbal treatments. Auto-immune hepatitis is associated with raised serum globulins (often >2x normal). Check auto-antibodies (ANA and smooth muscle Ab). Check -fetoprotein (elevated in primary hepatocellular cancer) particularly if suspicion of cirrhosis.
pain or jaundice and normal ultrasound
Ultrasound is the key test. If dilated bile ducts and no biliary type pain then likely to be malignant bile duct obstruction. Biliary-type pain and cholestatic liver tests requires urgent specialist review even if ultrasound normal. Most likely stones in common bile duct. ERCP or MRC may be required if diagnostic uncertainty. Consider drugs (see also below) Phenothiazines can continue if less than 2x normal. Remember stemetil may cause cholestasis. Augmentin and flucloxacillin may cause a progressive cholestasis with slow resolution over several months (after drug has been discontinued). Erythromycin may present as acute RUQ pain and may mimic cholecystitis. Non-specific cholestasis in sepsis and in chronic inflammatory conditions (e.g. inflammatory bowel disease). Congestive heart failure mild elevation (mixed picture) common with predominant right-sided heart failure related to hepatic congestion. Malignancy may be non-specific feature of disseminated cancer. Metastatic disease of the liver usually has a mixed pattern, mild elevations only; usually detected by ultrasound. Further examination by CT scan may be required particularly for solitary lesions. If chronic (> than six months) and progressive cholestasis consider chronic liver disorders such as primary biliary cirrhosis and sclerosing cholangitis. Specialist referral required for liver biopsy +/- ERCP. Order anti-mitochondrial antibody. Asymptomatic benign liver lesions (usually haemangiomas) are common and are not associated with liver test abnormalities.
Drugs and monitoring of liver enzymes
There are only a few examples of definite benefit from regular monitoring of liver enzymes: Isoniazid usually only transient elevation but must stop medication if progressive rise in liver enzymes (fulminant hepatitis may occur higher risk if >50 years). Methotrexate early elevation of AST/ALT in first few months may not be important; progressive changes may suggest hepatic fibrosis and need for liver biopsy. Azathioprine hepatitis may occur in first few months and require cessation of drug. 6-mercaptopurine may be a useful alternative. Cyproheptadine (used primarily for carcinoma of the prostate). Monthly liver enzymes in first few months stop if progressive elevation. Statins mild elevations of ALT common, particularly in first few months usually related to underlying fatty liver (there may be shifts in intra-hepatic lipids during initial treatment). Mild changes in LFTs do not predict serious liver disease and are not related to the risk of rhabdomyolysis.
Note 4: Check for evidence of impairment of hepatic function or portal hypertension (i.e. cirrhosis)
Important for all patients with chronic hepatitis. Check serum albumin and prothrombin ratio (even borderline abnormal levels are likely to be significant in the setting of chronic hepatitis). Thrombocytopenaenia suggests portal hypertension. Spleen may be enlarged but only detected by ultrasound.
Role of liver biopsy in investigation of abnormal liver tests
The majority of diagnoses are made by history (careful review of drug history), physical examination, and blood tests. For the few patients undiagnosed after usual blood tests (as above) liver biopsy may be indicated. In this situation the most common finding on liver biopsy is steatohepatitis (this may occur in absence of usual risk factors).
Note 5: Cholestasis pattern of elevated liver enzymes with no References
1. 2.
Competing interests
None declared.
Fraser A. Interpretation of liver enzyme tests a rapid guide. NZFP 2002; 29(2):117-120. Berkhan L. Interpretation of an elevated serum ferritin. NZFP 2002; 29(1):4548.
196
Volume 34 Number 3, June 2007
S-ar putea să vă placă și
- Understanding Acute and Chronic LeukemiaDocument10 paginiUnderstanding Acute and Chronic LeukemiaKrisha BalorioÎncă nu există evaluări
- Haematopathology 3:: Leucocytosis/LeucopeniaDocument113 paginiHaematopathology 3:: Leucocytosis/LeucopeniaarwaÎncă nu există evaluări
- CLINICAL CHEMISTRY: Passbooks Study GuideDe la EverandCLINICAL CHEMISTRY: Passbooks Study GuideÎncă nu există evaluări
- 1 Blood SmearDocument59 pagini1 Blood SmearGabi Tim100% (1)
- Decreased Levels of Iron by Diet or Hemorrhage Impaired Heme SynthesisDocument8 paginiDecreased Levels of Iron by Diet or Hemorrhage Impaired Heme SynthesisSamuel RothschildÎncă nu există evaluări
- Abnormal LFTsDocument2 paginiAbnormal LFTsRenu RosyÎncă nu există evaluări
- Uworld EndocrineDocument211 paginiUworld Endocrineهنادي رازمÎncă nu există evaluări
- Thalassemia and HaemoglobinopathiesDocument28 paginiThalassemia and HaemoglobinopathiesJared Khoo Er HauÎncă nu există evaluări
- Liver Function Tests Diagnostic GuideDocument2 paginiLiver Function Tests Diagnostic GuideostarburstoÎncă nu există evaluări
- Clinical Lab Hematology: An Overview of Blood Cell AnalysisDocument30 paginiClinical Lab Hematology: An Overview of Blood Cell AnalysisGerald SorianoÎncă nu există evaluări
- Observational Studies: Usmle Endpoint StatisticsDocument32 paginiObservational Studies: Usmle Endpoint Statisticskarim khalil100% (1)
- Molecular Diagnosis in HaematologyDocument23 paginiMolecular Diagnosis in HaematologyUmar'Farouq Oni100% (1)
- Acute Lymphoblastic Leukemia QuestionsDocument22 paginiAcute Lymphoblastic Leukemia Questionsđoàn lươngÎncă nu există evaluări
- Chart - WBC DisordersDocument1 paginăChart - WBC DisordersSamuel RothschildÎncă nu există evaluări
- Laboratory Tests For EndocrinologyDocument6 paginiLaboratory Tests For EndocrinologyAnastasia100% (1)
- Superficial and Cutaneous Mycoses: 2. Disease CharacteristicsDocument4 paginiSuperficial and Cutaneous Mycoses: 2. Disease CharacteristicsMA. ANGELI DELA CRUZÎncă nu există evaluări
- Hematology SummaryDocument9 paginiHematology SummaryJovielle Hayden100% (1)
- Hematology Review 2021-2Document142 paginiHematology Review 2021-2Maram AbdullahÎncă nu există evaluări
- Bone Marrow TransplantationDocument21 paginiBone Marrow TransplantationMorrison George100% (1)
- WBC Lymph Node SpleenDocument12 paginiWBC Lymph Node Spleendr brijesh TiwariÎncă nu există evaluări
- Chinese General Hospital Nursing College Functional Pattern GuideDocument2 paginiChinese General Hospital Nursing College Functional Pattern GuideTin BernardezÎncă nu există evaluări
- Stem Cell TransplantationDocument13 paginiStem Cell TransplantationMylls MondejarÎncă nu există evaluări
- Presented by T. V. L. Sahithi Ist Year PG Dept of PeriodonticsDocument49 paginiPresented by T. V. L. Sahithi Ist Year PG Dept of Periodonticslakshmi sahithi natakalaÎncă nu există evaluări
- End Indifference - Pope: Stray Bullet Cases Hit 36 Firecrackers Injure 459Document56 paginiEnd Indifference - Pope: Stray Bullet Cases Hit 36 Firecrackers Injure 459Art JasmeÎncă nu există evaluări
- 6 - ADKAR Reinforcement Ebook PDFDocument14 pagini6 - ADKAR Reinforcement Ebook PDFHenrique NarcisoÎncă nu există evaluări
- Basic Examination of Urine - Dr. PinedaDocument20 paginiBasic Examination of Urine - Dr. PinedaElei GarciaÎncă nu există evaluări
- Megaloblastic Anemia Testing AlgorithmDocument1 paginăMegaloblastic Anemia Testing AlgorithmkatÎncă nu există evaluări
- Liver Function Lecture NotesDocument9 paginiLiver Function Lecture NotesMarie Bernadette DigoÎncă nu există evaluări
- A Simple Guide to Hyperaldosteronism, Diagnosis, Treatment and Related ConditionsDe la EverandA Simple Guide to Hyperaldosteronism, Diagnosis, Treatment and Related ConditionsÎncă nu există evaluări
- Coagulation CascadeDocument4 paginiCoagulation CascadezainabÎncă nu există evaluări
- HepatosplenomegalyDocument52 paginiHepatosplenomegalySundar NatarajanÎncă nu există evaluări
- Hemodialysis Prescription and TreatmentDocument12 paginiHemodialysis Prescription and TreatmentkidneymastersÎncă nu există evaluări
- Abdul Rahim Bin Mohamad Nor C 111 10 871: Prof - Dr.Peter Kabo, PHD, SPFK, SPJP (K), Fiha, FasccDocument38 paginiAbdul Rahim Bin Mohamad Nor C 111 10 871: Prof - Dr.Peter Kabo, PHD, SPFK, SPJP (K), Fiha, FasccAis KonorasÎncă nu există evaluări
- Leukocyte DisordersDocument55 paginiLeukocyte DisordersSherlyn Yee100% (1)
- Lymphoid NeoplasmsDocument7 paginiLymphoid NeoplasmsMaribel SchullÎncă nu există evaluări
- Lebmc No. 67 Guidelines On Remote Classes For Class SuspensionDocument4 paginiLebmc No. 67 Guidelines On Remote Classes For Class SuspensionJoseB.JovellanoIIÎncă nu există evaluări
- HPLC PPT - KarishmaDocument76 paginiHPLC PPT - KarishmaDivya GauravÎncă nu există evaluări
- Saumya Gupta Moderator: Dr. Vishal GuptaDocument41 paginiSaumya Gupta Moderator: Dr. Vishal Guptaimranqazi11Încă nu există evaluări
- Board 4-CHNDocument30 paginiBoard 4-CHNKira100% (22)
- PhD Fluid MechanicsDocument4 paginiPhD Fluid MechanicsGooftilaaAniJiraachuunkooYesusiinÎncă nu există evaluări
- Unit Viii: The Hematologic SystemDocument1 paginăUnit Viii: The Hematologic SystemAqi RamenaiÎncă nu există evaluări
- UrinalysisDocument9 paginiUrinalysisSukma EffendyÎncă nu există evaluări
- Clin Path Trans 3.05 Urinalysis (2b)Document6 paginiClin Path Trans 3.05 Urinalysis (2b)Reymart FernandezÎncă nu există evaluări
- Red Cell and White Cell Counting, BloodDocument89 paginiRed Cell and White Cell Counting, BloodJovel GangcuangcoÎncă nu există evaluări
- Physical Examination of Urine: Analysis of Urine and Other Body Fluids Module 4Document19 paginiPhysical Examination of Urine: Analysis of Urine and Other Body Fluids Module 4Francis ValdezÎncă nu există evaluări
- Understanding Thalassemia: Causes, Symptoms and TreatmentDocument19 paginiUnderstanding Thalassemia: Causes, Symptoms and TreatmentJayricDepalobosÎncă nu există evaluări
- Acute Myeloid Leukemia in Children 2016Document10 paginiAcute Myeloid Leukemia in Children 2016Jorge Eduardo Espinoza RiosÎncă nu există evaluări
- Haematology - Blood Films.Document6 paginiHaematology - Blood Films.kkkssbbÎncă nu există evaluări
- Protein Metab 2 Dra. SantosDocument7 paginiProtein Metab 2 Dra. SantosMelissa SalayogÎncă nu există evaluări
- Cast in Urine SedimentDocument3 paginiCast in Urine Sedimentfirie100% (1)
- Goodpasture Syndrome: Lung and Kidney Autoimmune DiseaseDocument6 paginiGoodpasture Syndrome: Lung and Kidney Autoimmune DiseaseAman singhÎncă nu există evaluări
- Blood Conservation Methods in Anaesthesia and SurgeryDocument113 paginiBlood Conservation Methods in Anaesthesia and SurgeryAgya PrempehÎncă nu există evaluări
- Systemic Lupus Erythematosus Lecture Salah Abdel BakyDocument8 paginiSystemic Lupus Erythematosus Lecture Salah Abdel Bakyahmed gabrÎncă nu există evaluări
- RAAS CKD ProgressionDocument86 paginiRAAS CKD ProgressionNikesh DoshiÎncă nu există evaluări
- Argumentative EssayDocument24 paginiArgumentative EssayLiu166Încă nu există evaluări
- Chapter 13 Neoplastic Proliferations of White CellsDocument16 paginiChapter 13 Neoplastic Proliferations of White CellsOmar100% (1)
- HAEMOPOIESISDocument6 paginiHAEMOPOIESISDiyana ZahariÎncă nu există evaluări
- Macrocytic AnemiasDocument28 paginiMacrocytic AnemiasDeepankar SrigyanÎncă nu există evaluări
- Guide To Clinical Management of Idiopathic Pulmonary FibrosisDocument135 paginiGuide To Clinical Management of Idiopathic Pulmonary FibrosisConstantin PopescuÎncă nu există evaluări
- Pathophysiology 2Document92 paginiPathophysiology 2Princess AgarwalÎncă nu există evaluări
- Clearance and GFR: Major DR Arabinda Mohan Bhattarai Lecturer (Biochemistry), NAIHSDocument25 paginiClearance and GFR: Major DR Arabinda Mohan Bhattarai Lecturer (Biochemistry), NAIHSChandan SahÎncă nu există evaluări
- Hematology Lectures 1 5 DR - TuyDocument10 paginiHematology Lectures 1 5 DR - TuyMiguel Cuevas DolotÎncă nu există evaluări
- Hemolytic AnemiaDocument1 paginăHemolytic AnemiaTeus FatamorganaÎncă nu există evaluări
- Clinical Medicine - Lecture: - Topic: - DateDocument3 paginiClinical Medicine - Lecture: - Topic: - DateqselmmÎncă nu există evaluări
- Leukemia - Pathophysiology of White Cells DisordersDocument10 paginiLeukemia - Pathophysiology of White Cells DisordersJacecosmozÎncă nu există evaluări
- Polycythemia VeraDocument4 paginiPolycythemia VeraAllyson VillarÎncă nu există evaluări
- Red Blood Cell Anomalies: Elliptocytes & Oval MacrocyteDocument12 paginiRed Blood Cell Anomalies: Elliptocytes & Oval MacrocyteSHUPATUSSAI100% (1)
- CHR InflammationDocument33 paginiCHR InflammationAlnzeer6Încă nu există evaluări
- Carbapenem-Resistant Acinetobacter Baumannii Infections After Organ TransplantationDocument7 paginiCarbapenem-Resistant Acinetobacter Baumannii Infections After Organ TransplantationsserggiosÎncă nu există evaluări
- Fulminant Endocarditis and Disseminated Infection Caused by Carbapenem Resistant Acinetobacter Baumannii in A Renal Pancreas Transplant RecipientDocument8 paginiFulminant Endocarditis and Disseminated Infection Caused by Carbapenem Resistant Acinetobacter Baumannii in A Renal Pancreas Transplant RecipientsserggiosÎncă nu există evaluări
- Carbapenem-Resistant Enterobacteriaceae in Special Populations Solid Organ TransplantDocument13 paginiCarbapenem-Resistant Enterobacteriaceae in Special Populations Solid Organ TransplantsserggiosÎncă nu există evaluări
- Fulminant Endocarditis and Disseminated Infection Caused by Carbapenem Resistant Acinetobacter Baumannii in A Renal Pancreas Transplant RecipientDocument8 paginiFulminant Endocarditis and Disseminated Infection Caused by Carbapenem Resistant Acinetobacter Baumannii in A Renal Pancreas Transplant RecipientsserggiosÎncă nu există evaluări
- Evolution of Drug-Resistant Acinetobacter Baumannii After DCD Renal TransplantationDocument9 paginiEvolution of Drug-Resistant Acinetobacter Baumannii After DCD Renal TransplantationsserggiosÎncă nu există evaluări
- Evolution of Drug-Resistant Acinetobacter Baumannii After DCD Renal TransplantationDocument9 paginiEvolution of Drug-Resistant Acinetobacter Baumannii After DCD Renal TransplantationsserggiosÎncă nu există evaluări
- Carbapenem-Resistant Enterobacteriaceae in Special Populations Solid Organ TransplantDocument13 paginiCarbapenem-Resistant Enterobacteriaceae in Special Populations Solid Organ TransplantsserggiosÎncă nu există evaluări
- Epidemiology, Clinical Characteristics and Outcomes of Extensively Drug-Resistant Acinetobacter BaumanniiDocument10 paginiEpidemiology, Clinical Characteristics and Outcomes of Extensively Drug-Resistant Acinetobacter BaumanniisserggiosÎncă nu există evaluări
- Evolution of Drug-Resistant Acinetobacter Baumannii After DCD Renal TransplantationDocument9 paginiEvolution of Drug-Resistant Acinetobacter Baumannii After DCD Renal TransplantationsserggiosÎncă nu există evaluări
- Epidemiology, Clinical Characteristics and Outcomes of Extensively Drug-Resistant Acinetobacter BaumanniiDocument10 paginiEpidemiology, Clinical Characteristics and Outcomes of Extensively Drug-Resistant Acinetobacter BaumanniisserggiosÎncă nu există evaluări
- Carbapenem-Resistant Acinetobacter Baumannii Infections After Organ TransplantationDocument7 paginiCarbapenem-Resistant Acinetobacter Baumannii Infections After Organ TransplantationsserggiosÎncă nu există evaluări
- Fulminant Endocarditis and Disseminated Infection Caused by Carbapenem Resistant Acinetobacter Baumannii in A Renal Pancreas Transplant RecipientDocument8 paginiFulminant Endocarditis and Disseminated Infection Caused by Carbapenem Resistant Acinetobacter Baumannii in A Renal Pancreas Transplant RecipientsserggiosÎncă nu există evaluări
- Antibiotic Combination Effective Against Drug-Resistant BacteriaDocument7 paginiAntibiotic Combination Effective Against Drug-Resistant BacteriasserggiosÎncă nu există evaluări
- Antibiotic Combination Effective Against Drug-Resistant BacteriaDocument7 paginiAntibiotic Combination Effective Against Drug-Resistant BacteriasserggiosÎncă nu există evaluări
- Carbapenem-Resistant Enterobacteriaceae in Special Populations Solid Organ TransplantDocument13 paginiCarbapenem-Resistant Enterobacteriaceae in Special Populations Solid Organ TransplantsserggiosÎncă nu există evaluări
- Systematic Review of Metabolic Syndrome Biomarkers: A Panel For Early Detection, Management, and Risk Stratification in The West Virginian PopulationDocument14 paginiSystematic Review of Metabolic Syndrome Biomarkers: A Panel For Early Detection, Management, and Risk Stratification in The West Virginian PopulationDany RamdhaniÎncă nu există evaluări
- Carbapenem-Resistant Acinetobacter Baumannii Infections After Organ TransplantationDocument7 paginiCarbapenem-Resistant Acinetobacter Baumannii Infections After Organ TransplantationsserggiosÎncă nu există evaluări
- Nocardia Infection in KidneyDocument20 paginiNocardia Infection in KidneysserggiosÎncă nu există evaluări
- BMJ 336 7638 CR 00269Document4 paginiBMJ 336 7638 CR 00269sserggiosÎncă nu există evaluări
- A Retrospective Review at Two US TransplantDocument6 paginiA Retrospective Review at Two US TransplantsserggiosÎncă nu există evaluări
- Legionella Pneumophila PeritonitisDocument5 paginiLegionella Pneumophila PeritonitissserggiosÎncă nu există evaluări
- Reviews: The Spectrum of Celiac Disease: Epidemiology, Clinical Aspects and TreatmentDocument10 paginiReviews: The Spectrum of Celiac Disease: Epidemiology, Clinical Aspects and TreatmentsserggiosÎncă nu există evaluări
- Recent Advances and Clinical Outcomes of Kidney TransplantationDocument18 paginiRecent Advances and Clinical Outcomes of Kidney TransplantationsserggiosÎncă nu există evaluări
- Journal of Advanced Research: Usama A.A. Sharaf El Din, Mona M. Salem, Dina O. AbdulazimDocument12 paginiJournal of Advanced Research: Usama A.A. Sharaf El Din, Mona M. Salem, Dina O. AbdulazimNorman RiyadiÎncă nu există evaluări
- UK Standards for Microbiology Investigations: Detection of Enterobacteriaceae producing Extended Spectrum β-LactamasesDocument28 paginiUK Standards for Microbiology Investigations: Detection of Enterobacteriaceae producing Extended Spectrum β-LactamasessserggiosÎncă nu există evaluări
- Report of Twenty CasesDocument16 paginiReport of Twenty CasessserggiosÎncă nu există evaluări
- Kidney TransplantationDocument4 paginiKidney TransplantationsserggiosÎncă nu există evaluări
- The Molecular Investigation of Celiac DiseaseDocument7 paginiThe Molecular Investigation of Celiac DiseasesserggiosÎncă nu există evaluări
- Annsurg01228 0005Document12 paginiAnnsurg01228 0005sserggiosÎncă nu există evaluări
- Paper 1Document9 paginiPaper 1sserggiosÎncă nu există evaluări
- DelegationDocument24 paginiDelegationJP FernandezÎncă nu există evaluări
- NUR1204-RLE - Group 4 - Home Visit Activity (HTP and HVP)Document16 paginiNUR1204-RLE - Group 4 - Home Visit Activity (HTP and HVP)Jayvee BillonesÎncă nu există evaluări
- Lehane Histamine Scombroid ReportDocument84 paginiLehane Histamine Scombroid ReportGeraldine Pardo MariluzÎncă nu există evaluări
- 02 1975 Act DdbiaDocument13 pagini02 1975 Act DdbiaChuah C. KenÎncă nu există evaluări
- Study Online,: Graduate On CampusDocument28 paginiStudy Online,: Graduate On CampusattackcairoÎncă nu există evaluări
- 4 Answer On A Separate Sheet of Paper. Then Check Your Answers. Follow The ExamplesDocument5 pagini4 Answer On A Separate Sheet of Paper. Then Check Your Answers. Follow The ExamplesAndrea chaparroÎncă nu există evaluări
- The Relevance of Root Canal Isthmuses in Endodontic RehabilitationDocument13 paginiThe Relevance of Root Canal Isthmuses in Endodontic RehabilitationVictorÎncă nu există evaluări
- HezekiahWalters Plans 3Document34 paginiHezekiahWalters Plans 3Chris VaughnÎncă nu există evaluări
- Fungal Infection PicturesDocument26 paginiFungal Infection PicturesAshty RzgarÎncă nu există evaluări
- Peace Corps Violation of Office of Victim Advocate Clearances by OVA Employee DI-16-0254 WB CommentsDocument26 paginiPeace Corps Violation of Office of Victim Advocate Clearances by OVA Employee DI-16-0254 WB CommentsAccessible Journal Media: Peace Corps DocumentsÎncă nu există evaluări
- Dutra de Souza 2023Document11 paginiDutra de Souza 2023Paulo Emilio Marchete RohorÎncă nu există evaluări
- Ward D - Freida McFaddenDocument239 paginiWard D - Freida McFaddenHassan ZayanÎncă nu există evaluări
- BI Johor Paper1 (1) - SPMDocument3 paginiBI Johor Paper1 (1) - SPMrajpus08Încă nu există evaluări
- Pilar College Individual Nominee FormDocument2 paginiPilar College Individual Nominee FormDes CuenoÎncă nu există evaluări
- Therapeutic Communication: Prepared By: Mark Angelo C. Collado Kenneth Carl C. Roque Janella Rose Y. SusaDocument15 paginiTherapeutic Communication: Prepared By: Mark Angelo C. Collado Kenneth Carl C. Roque Janella Rose Y. SusaNashÎncă nu există evaluări
- 12 MR - Norhisam Omar, Sales Manager, South East Asia of TenCate Geosynthetics Asia SDN BHDDocument4 pagini12 MR - Norhisam Omar, Sales Manager, South East Asia of TenCate Geosynthetics Asia SDN BHDMuhammad FaisalÎncă nu există evaluări
- SelectionList R1 WebDocument586 paginiSelectionList R1 WebVishakha SutarÎncă nu există evaluări
- Interpreting PDX Dot BlotsDocument2 paginiInterpreting PDX Dot BlotsSpy CameraÎncă nu există evaluări
- Instructions For Treatment and Use of Insecticide-Treated Mosquito NetsDocument51 paginiInstructions For Treatment and Use of Insecticide-Treated Mosquito NetsMaxwell WrightÎncă nu există evaluări
- Plano FarmasiDocument44 paginiPlano FarmasiAna Cristina MachadoÎncă nu există evaluări
- Influence of Academic Work on SHS Students' Mental HealthDocument67 paginiInfluence of Academic Work on SHS Students' Mental HealthAliekfarsey Masukat100% (1)
- Cultural Differences in Travel Risk PerceptionDocument20 paginiCultural Differences in Travel Risk PerceptionEsther Charlotte Williams100% (2)