S-ar putea să vă placă și
- Oxycontin Marketing221Document7 paginiOxycontin Marketing221cetatiÎncă nu există evaluări
- Chapter 8 Infectious Diseases Robbins and Cotran Pathologic Basis of Disease PDFDocument12 paginiChapter 8 Infectious Diseases Robbins and Cotran Pathologic Basis of Disease PDFRitz Celso100% (1)
- Pharma CaseDocument20 paginiPharma CaseHaddadAkremÎncă nu există evaluări
- The Nervous System PDFDocument3 paginiThe Nervous System PDFPerry SinÎncă nu există evaluări
- The SOMATID - A Pleomorphic, Ultra-Microsopic Subcellular Living and Reproducing EntityDocument55 paginiThe SOMATID - A Pleomorphic, Ultra-Microsopic Subcellular Living and Reproducing EntityMarkMadMunkiÎncă nu există evaluări
- Iqvia Institute Global Oncology Trends 2022 ForwebDocument65 paginiIqvia Institute Global Oncology Trends 2022 ForwebYefinadya MfÎncă nu există evaluări
- Piramal DiagnosticsDocument12 paginiPiramal Diagnosticsanoozz100% (1)
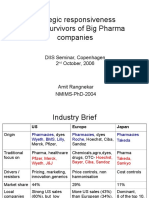
- Global Pharma StrategyDocument15 paginiGlobal Pharma StrategyDr Amit RangnekarÎncă nu există evaluări
- Sales Excellence in The Pharma IndustryDocument4 paginiSales Excellence in The Pharma IndustryKushal AgrawalÎncă nu există evaluări
- Global Oncology Trends 2018 PDFDocument64 paginiGlobal Oncology Trends 2018 PDFdrakchaturvedi100% (1)
- Lecture - Three (Pharma Marketing)Document44 paginiLecture - Three (Pharma Marketing)Sajid Ali MaariÎncă nu există evaluări
- Digital Strategies in PharmaDocument30 paginiDigital Strategies in Pharmajigar100% (1)
- Iqvia Institute Digital Health Trends 2021Document76 paginiIqvia Institute Digital Health Trends 2021Ivan IsaackÎncă nu există evaluări
- Lokesh Patil (22) - Madhura Jagtap (10) - Animesh Amal (01) - Vishal Mehta (16) - Khushbu MascarenhasDocument44 paginiLokesh Patil (22) - Madhura Jagtap (10) - Animesh Amal (01) - Vishal Mehta (16) - Khushbu MascarenhasAnonymous 75aETJ8OÎncă nu există evaluări
- Etizola Brand PlanDocument23 paginiEtizola Brand PlanMuhammad Ali JehangirÎncă nu există evaluări
- Strategyand Pharma Emerging Markets 2.0Document68 paginiStrategyand Pharma Emerging Markets 2.0VimalGarg100% (1)
- Opportunities and Challenges in An Evolving Market (KPMG)Document48 paginiOpportunities and Challenges in An Evolving Market (KPMG)vikalp123123Încă nu există evaluări
- Is Smart Pharma Innovative VFDocument28 paginiIs Smart Pharma Innovative VFvidya.sekarÎncă nu există evaluări
- Senior Director Oncology Marketing in USA Resume Mark MatthewsDocument2 paginiSenior Director Oncology Marketing in USA Resume Mark MatthewsMarkMatthewsÎncă nu există evaluări
- Presented by Animesh Amal: Brand Plan On Salbutamol + Ambroxol + GuaifenesinDocument36 paginiPresented by Animesh Amal: Brand Plan On Salbutamol + Ambroxol + GuaifenesinAnonymous 75aETJ8OÎncă nu există evaluări
- The Road To Digital Success in Pharma - McKinsey & CompanyDocument10 paginiThe Road To Digital Success in Pharma - McKinsey & CompanyharshalÎncă nu există evaluări
- Pharmaceutical MarketingDocument30 paginiPharmaceutical Marketingjudith sanicoÎncă nu există evaluări
- Pharma Field Force Excellence Special Issue - July 2012Document20 paginiPharma Field Force Excellence Special Issue - July 2012Anup SoansÎncă nu există evaluări
- Monitor Pharma Prescription Launches in Emerging Markets 083112Document28 paginiMonitor Pharma Prescription Launches in Emerging Markets 083112Siddharth SikariaÎncă nu există evaluări
- 1185916242Document60 pagini1185916242Mamimpin TambunanÎncă nu există evaluări
- Vipul Dholia RX To OTCDocument80 paginiVipul Dholia RX To OTCpooja_chowkseyÎncă nu există evaluări
- Zykast MKTDocument25 paginiZykast MKTkhanhquphamÎncă nu există evaluări
- Pharma AI SummitDocument10 paginiPharma AI Summitlinh nguyenÎncă nu există evaluări
- Test Bank For Human Anatomy 5th Edition MariebDocument18 paginiTest Bank For Human Anatomy 5th Edition MariebSandra Brown100% (5)
- Pharmaceutical Marketing: Marketing Strategy Alternative Strategic ThrustsDocument29 paginiPharmaceutical Marketing: Marketing Strategy Alternative Strategic Thrustspremoshin100% (4)
- Global Oncology Trends 2021-2025Document70 paginiGlobal Oncology Trends 2021-2025Deepak MakkarÎncă nu există evaluări
- Personal Selling in Pharma Marketing: Shilpa GargDocument17 paginiPersonal Selling in Pharma Marketing: Shilpa GargNikhil MahajanÎncă nu există evaluări
- Emilok Marketing Plan 2017Document38 paginiEmilok Marketing Plan 2017maawi2002yahoocomÎncă nu există evaluări
- Scientific Advice Meetings: A Guide to Successful Interactions with FDA, EMA and BeyondDe la EverandScientific Advice Meetings: A Guide to Successful Interactions with FDA, EMA and BeyondÎncă nu există evaluări
- Zuellig Pharma Annual Magazine 2019Document18 paginiZuellig Pharma Annual Magazine 2019James VillegasÎncă nu există evaluări
- Medical AffairsDocument11 paginiMedical Affairssightbd0% (1)
- Indian Diagnostic Services Market Outlook 2020: BrochureDocument6 paginiIndian Diagnostic Services Market Outlook 2020: BrochureBalachandar SeemanÎncă nu există evaluări
- Managing Human Resources 8th EditionDocument3 paginiManaging Human Resources 8th Editioncookiebgood0% (14)
- Breast Cancer Market1Document9 paginiBreast Cancer Market1anilpharma102Încă nu există evaluări
- Oncology PipelinesDocument92 paginiOncology PipelinesvczeszynÎncă nu există evaluări
- IBM Case Study in PharmaDocument16 paginiIBM Case Study in PharmasupriyoÎncă nu există evaluări
- Ashraf Shahin EGPIDocument28 paginiAshraf Shahin EGPIAshraf ShahinÎncă nu există evaluări
- Patient Journey Mapping: With An Example of Diabetic ClinicDocument4 paginiPatient Journey Mapping: With An Example of Diabetic Clinicvijaya lakshmiÎncă nu există evaluări
- Prepared by Muhammad Salman: This Brand Plan Has Been Designed For The ProductDocument73 paginiPrepared by Muhammad Salman: This Brand Plan Has Been Designed For The ProductMuhammad SalmanÎncă nu există evaluări
- Forecasting Pharma Ind Book BrochureDocument2 paginiForecasting Pharma Ind Book BrochureAbhishek DixitÎncă nu există evaluări
- Case Study DR Reddy-Industry PDFDocument61 paginiCase Study DR Reddy-Industry PDFSyed0% (2)
- Accenture Five Branded Generics Strategies Pharmaceuticals in Emerging MarketsDocument16 paginiAccenture Five Branded Generics Strategies Pharmaceuticals in Emerging MarketsAnonymous 75aETJ8OÎncă nu există evaluări
- Territory Sales Manager Medical Device in San Antonio TX Resume Andrew RowlandsDocument2 paginiTerritory Sales Manager Medical Device in San Antonio TX Resume Andrew RowlandsAndrewRowlandsÎncă nu există evaluări
- Pricing Strategies in HealthcareDocument4 paginiPricing Strategies in HealthcareAvantika ChaudharyÎncă nu există evaluări
- Branding & Positioning in HealthcareDocument86 paginiBranding & Positioning in HealthcaresudhakerjadhavÎncă nu există evaluări
- Challenges and Caveats in Oncology ForecastingDocument4 paginiChallenges and Caveats in Oncology ForecastingmaleticjÎncă nu există evaluări
- Thrombocytopenia in CLD - Market Access Landscape - Interim - 16012015Document60 paginiThrombocytopenia in CLD - Market Access Landscape - Interim - 16012015Pranjal SahaiÎncă nu există evaluări
- Roland Berger - Pharmaceutical Industry Study 2009 - What Is NextDocument40 paginiRoland Berger - Pharmaceutical Industry Study 2009 - What Is Nextapritul3539Încă nu există evaluări
- Case Study Leadership Booster Shot For GSK Pharmaceuticals KNOLSKAPEDocument4 paginiCase Study Leadership Booster Shot For GSK Pharmaceuticals KNOLSKAPEHardik ChitrodaÎncă nu există evaluări
- Research Report - Dr. Reddy'sDocument8 paginiResearch Report - Dr. Reddy'sDishant KhanejaÎncă nu există evaluări
- Deloitte Personalised Medicine Analysis-PGx-ROIDocument32 paginiDeloitte Personalised Medicine Analysis-PGx-ROISimranjit SinghÎncă nu există evaluări
- Questions Before LaunchDocument3 paginiQuestions Before LaunchPerri CebedoÎncă nu există evaluări
- Roland Berger - Pharmaceutical Industry Study 2012 - Fight For ProfitabilityDocument44 paginiRoland Berger - Pharmaceutical Industry Study 2012 - Fight For Profitabilityapritul3539Încă nu există evaluări
- Path Lab 19-20 PDFDocument202 paginiPath Lab 19-20 PDFPriyesh Bharad0% (1)
- CH01 Printer PDFDocument26 paginiCH01 Printer PDFClaire Evann Villena EboraÎncă nu există evaluări
- RX OTC Switch FlyerDocument4 paginiRX OTC Switch FlyerbhaskarnisÎncă nu există evaluări
- Epidemiology Based Market ForecastDocument7 paginiEpidemiology Based Market Forecastkarthi339Încă nu există evaluări
- Johnson & Johnson: "Caring For You From The Beginning, To The Very End!"Document18 paginiJohnson & Johnson: "Caring For You From The Beginning, To The Very End!"Kaushik BalachandarÎncă nu există evaluări
- Bayer Capital Day 2021Document6 paginiBayer Capital Day 2021BDÎncă nu există evaluări
- Cancer Growth Inhibitors Market & Clinical Pipeline AnalDocument7 paginiCancer Growth Inhibitors Market & Clinical Pipeline AnalNeeraj Chawla100% (1)
- Jurkat, Clone E6 1 (ATCC TIB 152) : Product SheetDocument3 paginiJurkat, Clone E6 1 (ATCC TIB 152) : Product Sheetabdul88fÎncă nu există evaluări
- Lab ReviewerDocument3 paginiLab Reviewerryana cabreraÎncă nu există evaluări
- Biology 1010 General ObjectivesDocument2 paginiBiology 1010 General Objectivesapi-241247043Încă nu există evaluări
- Peripheral Neuropathy Associated With Mitochondrial Disease in ChildrenDocument8 paginiPeripheral Neuropathy Associated With Mitochondrial Disease in ChildrenRenata CardosoÎncă nu există evaluări
- Genetic EngineeringDocument14 paginiGenetic Engineering4L Anisha SieudassÎncă nu există evaluări
- Tife Chapter Two-2Document37 paginiTife Chapter Two-2Ajegbomogun SundayÎncă nu există evaluări
- 269 - Embryology Physiology) Development of The Heart  - ÏDocument11 pagini269 - Embryology Physiology) Development of The Heart  - ÏFood Safety CommunityÎncă nu există evaluări
- Staphylococcus Aureus Biofilms Interfere With Macrophage AntimicrDocument175 paginiStaphylococcus Aureus Biofilms Interfere With Macrophage AntimicrshalusinhaÎncă nu există evaluări
- CH 12Document9 paginiCH 12lalitÎncă nu există evaluări
- KARYOTYPEDocument23 paginiKARYOTYPELucia AndreeaÎncă nu există evaluări
- IdmDocument46 paginiIdmht8zwk946sÎncă nu există evaluări
- CauliflowerDocument4 paginiCauliflowerIzhar Ahmad DanishÎncă nu există evaluări
- LunaDocument24 paginiLunaapi-471513506Încă nu există evaluări
- 2019 32 Notifn Vet Asst SurgDocument26 pagini2019 32 Notifn Vet Asst SurgThiru NavukarasuÎncă nu există evaluări
- Lesson 4 Infancy by HurlockDocument44 paginiLesson 4 Infancy by HurlockJessica Recaido100% (1)
- Special Access List of Covid-19 Test Kit (For Professional Use Only)Document2 paginiSpecial Access List of Covid-19 Test Kit (For Professional Use Only)Devina FernsÎncă nu există evaluări
- Aplastic Hemolitic 2021 OlgaDocument43 paginiAplastic Hemolitic 2021 OlgalaibaÎncă nu există evaluări
- Ria ImmunoassayDocument10 paginiRia ImmunoassayDinkey SharmaÎncă nu există evaluări
- Nurse Writing 003 OET Practice Letter by PASS OETDocument26 paginiNurse Writing 003 OET Practice Letter by PASS OETNajad Salahudeen50% (2)
- Biology SL P2Document8 paginiBiology SL P2KenanÎncă nu există evaluări
- Can Genes Predict Athletic Performance?Document2 paginiCan Genes Predict Athletic Performance?Channy PhamÎncă nu există evaluări
- T1-2P1 MSDocument28 paginiT1-2P1 MSVladimir TrajanovikjÎncă nu există evaluări
- Biological Impact of Feeding Rats With A Genetically Modified-Based DietDocument11 paginiBiological Impact of Feeding Rats With A Genetically Modified-Based DietJesús Rafael Méndez NateraÎncă nu există evaluări
- 5Document3 pagini5Nidhi JaisÎncă nu există evaluări
- Early HumanDocument4 paginiEarly HumanPeem JatabutÎncă nu există evaluări