S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Flanigan MaleGUDocument28 paginiFlanigan MaleGUdidu91Încă nu există evaluări
- Comorbiditari ADHD I. ADHD in Adults-What Science SaysDocument2 paginiComorbiditari ADHD I. ADHD in Adults-What Science Saysdidu91Încă nu există evaluări
- Physical Diagnosis in OtolaryngologyDocument32 paginiPhysical Diagnosis in Otolaryngologydidu91Încă nu există evaluări
- Mus Culo SkeletalDocument48 paginiMus Culo Skeletaldidutza91Încă nu există evaluări
- Abdomen ExaminationDocument59 paginiAbdomen Examinationbenmanu2009Încă nu există evaluări
- CodependencyDocument1 paginăCodependencydidu91Încă nu există evaluări
- Stress Busting DiaryDocument1 paginăStress Busting Diarydidu91Încă nu există evaluări
- Case Presentation: Male HypogonadismDocument17 paginiCase Presentation: Male Hypogonadismdidu91Încă nu există evaluări
- Case Presentation: Hirsutism and OligomenorrheaDocument20 paginiCase Presentation: Hirsutism and Oligomenorrheadidu91Încă nu există evaluări
- Emotional Intelligence Toolkit Stress Busting DiaryDocument1 paginăEmotional Intelligence Toolkit Stress Busting Diarydidu91Încă nu există evaluări
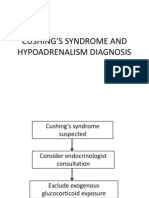
- Cushing'S Syndrome and Hypoadrenalism DiagnosisDocument29 paginiCushing'S Syndrome and Hypoadrenalism Diagnosisdidu91Încă nu există evaluări
- Pheochromocytoma-A Case PresentationDocument14 paginiPheochromocytoma-A Case Presentationdidu91Încă nu există evaluări
- Acromegaly: Case ReportDocument22 paginiAcromegaly: Case Reportdidu91Încă nu există evaluări
- Thyroid Gland: Pactical Activity No. 5Document19 paginiThyroid Gland: Pactical Activity No. 5didu91Încă nu există evaluări
- C. D, 43 Years, Male First Admission in Our Department in September 2012Document18 paginiC. D, 43 Years, Male First Admission in Our Department in September 2012didu91Încă nu există evaluări
- Thyroid Cancer: Case ReportDocument19 paginiThyroid Cancer: Case Reportdidu91Încă nu există evaluări
- Basedow-Graves Disease: A Case PresentationDocument12 paginiBasedow-Graves Disease: A Case Presentationdidu91Încă nu există evaluări
- Case Presentation: Short Stature and Pubertal DelayDocument27 paginiCase Presentation: Short Stature and Pubertal Delaydidu91Încă nu există evaluări
- Pituitary Tumor Syndrome Diabetes Insipidus: Case ReportDocument25 paginiPituitary Tumor Syndrome Diabetes Insipidus: Case Reportdidu91Încă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- LifeCare DeraDocument13 paginiLifeCare Derasandeep singh cheemaÎncă nu există evaluări
- Kadali Et Al Non Life Threatening Adverse Effects ModernaDocument10 paginiKadali Et Al Non Life Threatening Adverse Effects ModernaJoshua TamayoÎncă nu există evaluări
- Types of IncisionsDocument6 paginiTypes of IncisionsKim GomezÎncă nu există evaluări
- Cardiac RehabilitationDocument48 paginiCardiac RehabilitationsdsdÎncă nu există evaluări
- Aortic Valve RegurgitationDocument3 paginiAortic Valve RegurgitationMarky StrikerÎncă nu există evaluări
- Human Anatomy and Physiology Laboratory Manual Fetal Pig Version Update 10Th Edition Marieb Test Bank Full Chapter PDFDocument33 paginiHuman Anatomy and Physiology Laboratory Manual Fetal Pig Version Update 10Th Edition Marieb Test Bank Full Chapter PDFAlexandraPerrymzyd100% (10)
- MtSinai PatientGuideDocument40 paginiMtSinai PatientGuideobada alrefaiÎncă nu există evaluări
- INOTROPESDocument8 paginiINOTROPESessevyÎncă nu există evaluări
- Case Emfisema ParuDocument3 paginiCase Emfisema ParuMuhammad SyukurÎncă nu există evaluări
- Abnormal ECGDocument55 paginiAbnormal ECGdevilbata50% (2)
- Buerger's DiseaseDocument8 paginiBuerger's DiseaseELSA HANA AL MUNAWAROHÎncă nu există evaluări
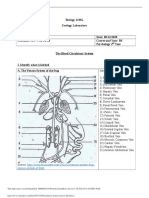
- Circulatory System Answer SheetDocument4 paginiCirculatory System Answer SheetMarlie TobiseÎncă nu există evaluări
- The Effects of SmokingDocument2 paginiThe Effects of SmokingNino-prexy AcdalÎncă nu există evaluări
- Chapter 18 - Liver and Biliary TractDocument18 paginiChapter 18 - Liver and Biliary TractAgnieszka WisniewskaÎncă nu există evaluări
- 10.2 - RheumatologyDocument40 pagini10.2 - Rheumatologyayeshafarooq60Încă nu există evaluări
- Rat & Mouse Carotid Artery Acute Blood Flow (RL-62-sp)Document3 paginiRat & Mouse Carotid Artery Acute Blood Flow (RL-62-sp)nilberto2Încă nu există evaluări
- Science Quiz Bee ReviewerDocument26 paginiScience Quiz Bee ReviewerCatherine Joy Dela Cruz92% (13)
- Hepatic, Pancreatic, and Rare Gastrointestinal Complications of Immune Checkpoint Inhibitor Therapy - UpToDateDocument29 paginiHepatic, Pancreatic, and Rare Gastrointestinal Complications of Immune Checkpoint Inhibitor Therapy - UpToDatemayteveronica1000Încă nu există evaluări
- Ischaemia of Lower Limbs: by Dr. ShampileDocument46 paginiIschaemia of Lower Limbs: by Dr. ShampileFreeburn SimunchembuÎncă nu există evaluări
- Reviewer #1 (Sir Labajo)Document10 paginiReviewer #1 (Sir Labajo)Marivy GalonÎncă nu există evaluări
- Heart Sound AnalysisDocument41 paginiHeart Sound AnalysisSoham RoyÎncă nu există evaluări
- Pointers To ReviewDocument8 paginiPointers To Reviewjoan ruby bautistaÎncă nu există evaluări
- Vascularizatia SNCDocument106 paginiVascularizatia SNCCiopraga IuliaÎncă nu există evaluări
- Heart MafiaDocument1 paginăHeart Mafiaastf mahboobÎncă nu există evaluări
- Pleura Its ReflectionsDocument52 paginiPleura Its Reflectionskasozi marvinÎncă nu există evaluări
- HAP Chapterwise MCQ For 2nd Sessional PDFDocument6 paginiHAP Chapterwise MCQ For 2nd Sessional PDFsaurav prasadÎncă nu există evaluări
- ArrhythmiasDocument23 paginiArrhythmiasKelvin Mandela100% (1)
- Komplikasi Pada Pasien Infark Miokard Akut ST-Elevasi (STEMI) Yang Mendapat Maupun Tidak Mendapat Terapi Reperfu..Document13 paginiKomplikasi Pada Pasien Infark Miokard Akut ST-Elevasi (STEMI) Yang Mendapat Maupun Tidak Mendapat Terapi Reperfu..aris hidayatul mÎncă nu există evaluări
- Drug Study For PneumoniaDocument15 paginiDrug Study For PneumoniaPrincess Pauline Abrasaldo100% (1)
- Kidneys: LocationDocument6 paginiKidneys: LocationRanjana Das BhowmickÎncă nu există evaluări