S-ar putea să vă placă și
- Gout Lecture PDFDocument9 paginiGout Lecture PDFYantimuliawatiÎncă nu există evaluări
- Crystal Deposition Disorders ReviewDocument68 paginiCrystal Deposition Disorders ReviewMustafa Abbas AlObaidyÎncă nu există evaluări
- Management of hyperuricemia and gouty arthritis with Unani medicine and wet cuppingDocument4 paginiManagement of hyperuricemia and gouty arthritis with Unani medicine and wet cuppingDharma Yoga Ayurveda MassageÎncă nu există evaluări
- Gout and HyperuricemiaDocument70 paginiGout and HyperuricemiaThe AbyssinicansÎncă nu există evaluări
- Chronic Hyperuricemia, Uric Acid Deposit and Cardiovascular RiskDocument7 paginiChronic Hyperuricemia, Uric Acid Deposit and Cardiovascular RiskBelleÎncă nu există evaluări
- Gout 130718051351 Phpapp01Document47 paginiGout 130718051351 Phpapp01Manurun Londong AlloÎncă nu există evaluări
- Notes For Cc2 FeportDocument3 paginiNotes For Cc2 FeportKhisha RangasÎncă nu există evaluări
- 1 GoutDocument5 pagini1 Goutiraqeana100100Încă nu există evaluări
- Diagnosis and Treatment of Gout and PseudogoutDocument24 paginiDiagnosis and Treatment of Gout and PseudogoutPutri Aswariyah RamliÎncă nu există evaluări
- Pancreas Enzyme SecretionDocument7 paginiPancreas Enzyme SecretionJuan Carlos LunaÎncă nu există evaluări
- Clinpharm M4 ReviewerDocument10 paginiClinpharm M4 ReviewerCHARLES RONALD GENATOÎncă nu există evaluări
- Understanding Uric Acid: Biochemistry, Physiology, and Clinical SignificanceDocument28 paginiUnderstanding Uric Acid: Biochemistry, Physiology, and Clinical SignificanceAya100% (1)
- Differential diagnoses of joint pain scenarioDocument9 paginiDifferential diagnoses of joint pain scenarioNUR ZAMZAM AZIZAHÎncă nu există evaluări
- Uric Acid ProductionDocument21 paginiUric Acid ProductionNeha Srivastava0% (1)
- Crystal Induced Arthropathies: BY: DR Mehrunnisa Umar Assisstant Profesor Department of MedicineDocument25 paginiCrystal Induced Arthropathies: BY: DR Mehrunnisa Umar Assisstant Profesor Department of MedicinedrusmanjamilhcmdÎncă nu există evaluări
- GOUT AND PSEUDOGOUT: CRYSTAL-ASSOCIATED ARTHRITISDocument56 paginiGOUT AND PSEUDOGOUT: CRYSTAL-ASSOCIATED ARTHRITISSindhu BabuÎncă nu există evaluări
- HyperuricemiaDocument10 paginiHyperuricemianinroseÎncă nu există evaluări
- Is There A Pathogenetic Role For Uric Acid in Hypertension and Cardiovascular and Renal Disease?Document9 paginiIs There A Pathogenetic Role For Uric Acid in Hypertension and Cardiovascular and Renal Disease?Rachel AritonangÎncă nu există evaluări
- Gout and HyperuricaemiaDocument57 paginiGout and HyperuricaemiaAmer JumahÎncă nu există evaluări
- Uric Acid Determination PDFDocument10 paginiUric Acid Determination PDFJhon Jerome DapdapÎncă nu există evaluări
- Lec 2Document7 paginiLec 2Sajjad FalahÎncă nu există evaluări
- Disorders of Adrenal GlandsDocument48 paginiDisorders of Adrenal GlandsCharlz ZipaganÎncă nu există evaluări
- Acute Renal FailureDocument25 paginiAcute Renal FailurenyarieÎncă nu există evaluări
- Uric AcidDocument13 paginiUric Acidphoto copyhemnÎncă nu există evaluări
- Hepatological Diseases in AnimalsDocument34 paginiHepatological Diseases in AnimalsRICHARD RODERICK OLMEDOÎncă nu există evaluări
- Gout and Purine Degradation: Arun.SDocument7 paginiGout and Purine Degradation: Arun.SarunÎncă nu există evaluări
- DRUG-INDUCED HYPERURICEMIA AND GOUTDocument3 paginiDRUG-INDUCED HYPERURICEMIA AND GOUTAnggun Cahya MertyanaÎncă nu există evaluări
- Disorders of Purine Nucleotide MetabolismDocument3 paginiDisorders of Purine Nucleotide MetabolismPraiseÎncă nu există evaluări
- 5 - Drugs Used For Treatment of Gout EditedDocument35 pagini5 - Drugs Used For Treatment of Gout EditedSakariye hasanÎncă nu există evaluări
- Acute Renal Failure & Chronic Renal FailureDocument39 paginiAcute Renal Failure & Chronic Renal FailureMarie MayÎncă nu există evaluări
- Uric Acid1Document18 paginiUric Acid1Mustafa KhandgawiÎncă nu există evaluări
- Akram Et AlDocument3 paginiAkram Et AlElok IzawatiÎncă nu există evaluări
- GoutDocument5 paginiGoutDe Sesto Rhys Carlo100% (2)
- Acute Renal Failure Definition and CausesDocument33 paginiAcute Renal Failure Definition and Causesimranqazi11Încă nu există evaluări
- Crystal Deposition DisordersDocument4 paginiCrystal Deposition DisordersShuvashishSunuwarÎncă nu există evaluări
- Kidney Disease by Rehana Mam.Document22 paginiKidney Disease by Rehana Mam.raisameh23Încă nu există evaluări
- Adrenal Gland Disorders ExplainedDocument73 paginiAdrenal Gland Disorders ExplainedReunita ConstantiaÎncă nu există evaluări
- Non-Protein Nitrogen CompoundsDocument6 paginiNon-Protein Nitrogen CompoundspixiedustÎncă nu există evaluări
- Essential Notes For The MRCP 3rd PDFDocument613 paginiEssential Notes For The MRCP 3rd PDFnayhtun2471100% (1)
- The Parathyroid GlandsDocument6 paginiThe Parathyroid GlandsWinnie Salazar AriolaÎncă nu există evaluări
- Cirrhosis: Etiology, Complications, TreatmentDocument5 paginiCirrhosis: Etiology, Complications, TreatmentNahanÎncă nu există evaluări
- Etiology and Pathogenesis of GoutDocument13 paginiEtiology and Pathogenesis of GoutDaniÎncă nu există evaluări
- L9 - Biliary EnzymesDocument21 paginiL9 - Biliary Enzymesyouservezeropurpose113Încă nu există evaluări
- Chapter III. GoutDocument28 paginiChapter III. GoutWilliam C ChishaÎncă nu există evaluări
- GOUT PresentationDocument24 paginiGOUT Presentationtasneemsofi100% (1)
- Okell MedicineDocument300 paginiOkell MedicinePeprah Ondiba100% (2)
- Low purine diet reduces uric acidDocument3 paginiLow purine diet reduces uric acidRichel Edwin Theofili PattikawaÎncă nu există evaluări
- Clinically Important Enzymes and Diagnostic Application Class 2 2012 (المحاضره الخامسه)Document21 paginiClinically Important Enzymes and Diagnostic Application Class 2 2012 (المحاضره الخامسه)Anisam AbhiÎncă nu există evaluări
- Pharmacology Test 3 ReviewDocument6 paginiPharmacology Test 3 ReviewNatalia BortellÎncă nu există evaluări
- REVIEW 2023 AUBF Basics On Chemical Tests For UrineDocument84 paginiREVIEW 2023 AUBF Basics On Chemical Tests For UrineJheshari VinaÎncă nu există evaluări
- FrancesFranciscoCC2 1Document6 paginiFrancesFranciscoCC2 1Frances FranciscoÎncă nu există evaluări
- Non Viral HepatitisDocument40 paginiNon Viral Hepatitisostaz2000100% (1)
- ACUTE RENAL FAILURE DIAGNOSIS & MANAGEMENTDocument2 paginiACUTE RENAL FAILURE DIAGNOSIS & MANAGEMENTSetiya Dini LarasatiÎncă nu există evaluări
- Drug Induced Hepatitis: Dr.M.Sharmila Assistant Professor M7 (Prof CR Unit) Institute of Internal MedicineDocument21 paginiDrug Induced Hepatitis: Dr.M.Sharmila Assistant Professor M7 (Prof CR Unit) Institute of Internal MedicineAtakan Yeşil100% (1)
- Understanding and Treating GoutDocument6 paginiUnderstanding and Treating GoutJokevin PrasetyadhiÎncă nu există evaluări
- OUM Tutorial 1 SBNS3504 RenalDocument51 paginiOUM Tutorial 1 SBNS3504 RenalMashanimy HoneyÎncă nu există evaluări
- Hyper Ure Semi ADocument44 paginiHyper Ure Semi Abagusputrabali13Încă nu există evaluări
- Anti Gout: by Dr. Saba TariqDocument32 paginiAnti Gout: by Dr. Saba TariqDr. Saba TariqÎncă nu există evaluări
- The Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionDe la EverandThe Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionÎncă nu există evaluări
- Molybdenum Disulfide: A New Filter That Can Revolutionise Water Treatment by Yusuf AddanDocument10 paginiMolybdenum Disulfide: A New Filter That Can Revolutionise Water Treatment by Yusuf AddanSaaqo QasimÎncă nu există evaluări
- Estimating UncertaintyDocument4 paginiEstimating UncertaintySaaqo QasimÎncă nu există evaluări
- Acids & Alkalis Information BookletDocument14 paginiAcids & Alkalis Information BookletSaaqo QasimÎncă nu există evaluări
- Acids and AlkalisDocument37 paginiAcids and AlkalisSaaqo QasimÎncă nu există evaluări
- 1303 KSA Tutor Fellow Info PackDocument16 pagini1303 KSA Tutor Fellow Info PackSaaqo QasimÎncă nu există evaluări
- Plasma Proteins in Disease DiagnosisDocument81 paginiPlasma Proteins in Disease DiagnosisSaaqo Qasim100% (1)
- ACN Customer Acquisition StrategiesDocument15 paginiACN Customer Acquisition StrategiesSaaqo QasimÎncă nu există evaluări
- Lesson PlanDocument2 paginiLesson PlanSaaqo QasimÎncă nu există evaluări
- Alkynes: Properties of Compounds with Triple Carbon BondsDocument10 paginiAlkynes: Properties of Compounds with Triple Carbon BondsSaaqo QasimÎncă nu există evaluări
- Example of A Good Biotech EssayDocument7 paginiExample of A Good Biotech EssaySaaqo QasimÎncă nu există evaluări
- Separation Techniques Student Sheet: Intended Lesson OutcomesDocument19 paginiSeparation Techniques Student Sheet: Intended Lesson Outcomeslianchen251110Încă nu există evaluări
- 9701 Y13 SyDocument104 pagini9701 Y13 SySaaqo QasimÎncă nu există evaluări
- Physics Workbook 2011-2012Document45 paginiPhysics Workbook 2011-2012Pablo SilvaÎncă nu există evaluări
- Aggregate Crushing Plant GuideDocument24 paginiAggregate Crushing Plant GuideVineet AgrawalÎncă nu există evaluări
- Brown 2010 LoDocument4 paginiBrown 2010 LoSaaqo QasimÎncă nu există evaluări
- Elements Mixtures Compounds LessonDocument5 paginiElements Mixtures Compounds LessonSaaqo QasimÎncă nu există evaluări
- Intracellular Ca Signalling: Ca Influx Dr. Anant B. ParekhDocument17 paginiIntracellular Ca Signalling: Ca Influx Dr. Anant B. ParekhSaaqo QasimÎncă nu există evaluări
- 1303 KSA Tutor Fellow Info PackDocument16 pagini1303 KSA Tutor Fellow Info PackSaaqo QasimÎncă nu există evaluări
- 6CH01 ErDocument34 pagini6CH01 ErHussain MustafaÎncă nu există evaluări
- Aqa Byb5w W QP Jun06Document16 paginiAqa Byb5w W QP Jun06Saaqo Qasim0% (1)
- Roles of TGFβ in metastasisDocument14 paginiRoles of TGFβ in metastasisSaaqo QasimÎncă nu există evaluări
- Viruses 02 00166Document23 paginiViruses 02 00166Saaqo QasimÎncă nu există evaluări
- Clinical and Microbiology SSIDocument6 paginiClinical and Microbiology SSIFaozan FikriÎncă nu există evaluări
- Drug-Addiction-Biology ProjectDocument37 paginiDrug-Addiction-Biology ProjectAhalya Bai SahooÎncă nu există evaluări
- 200+ One-word substitutionsDocument10 pagini200+ One-word substitutionsRaktimÎncă nu există evaluări
- Omasoabomasal Impaction in A Gersy CowDocument6 paginiOmasoabomasal Impaction in A Gersy CowAli H. Sadiek أ.د. علي حسن صديق100% (1)
- Descartes Error PDFDocument15 paginiDescartes Error PDFstewatia100% (2)
- Essential Principles of Food Safety ManagementDocument342 paginiEssential Principles of Food Safety ManagementSanath KamilaÎncă nu există evaluări
- PN Comprehensive Practice A Anad B Questions and Answers VerifiedDocument8 paginiPN Comprehensive Practice A Anad B Questions and Answers Verifiedianshirow834Încă nu există evaluări
- 3 My Case StudyDocument6 pagini3 My Case StudyAnimroslan AnimÎncă nu există evaluări
- Thyrocare PrezDocument18 paginiThyrocare PrezDr Amit RangnekarÎncă nu există evaluări
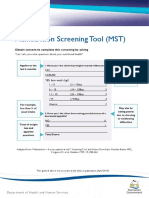
- Malnutrition Screening Tool (MSTDocument2 paginiMalnutrition Screening Tool (MSTAku dienaÎncă nu există evaluări
- Exercise Therapy For Muscle and Lower Motor Neuron Diseases: Aisha Munawar Sheikh, John VissingDocument18 paginiExercise Therapy For Muscle and Lower Motor Neuron Diseases: Aisha Munawar Sheikh, John VissingTito AlhoÎncă nu există evaluări
- The Adrenal Thyroid Revolution Supplement Guide: SOS RX: Daily Dose SupplementsDocument8 paginiThe Adrenal Thyroid Revolution Supplement Guide: SOS RX: Daily Dose SupplementsPetra JobovaÎncă nu există evaluări
- Noun ClassesDocument51 paginiNoun ClassesAvrahamÎncă nu există evaluări
- CSP - Groin LumpDocument39 paginiCSP - Groin LumpAnnisa SakilaÎncă nu există evaluări
- Reflecting on Insanity and Freedom in One Flew Over Cuckoo's NestDocument2 paginiReflecting on Insanity and Freedom in One Flew Over Cuckoo's NestAnna Oh40% (5)
- LEPTOSPIROSIS PowerPointDocument10 paginiLEPTOSPIROSIS PowerPointAmira Bint KhalidÎncă nu există evaluări
- Summative Test in Health 7Document2 paginiSummative Test in Health 7Myra Iligan0% (1)
- (Jurnal) Sonography in Male InfertilityDocument25 pagini(Jurnal) Sonography in Male InfertilityIrni Dwi Aprianty IbrahimÎncă nu există evaluări
- Health Q3 M2Document15 paginiHealth Q3 M2olameonfrixandrei486Încă nu există evaluări
- EweDocument246 paginiEweOluwo88% (32)
- Peace Corps Report of Dental Examination - PC-OMS-1790 Dental 08/2009Document4 paginiPeace Corps Report of Dental Examination - PC-OMS-1790 Dental 08/2009Accessible Journal Media: Peace Corps DocumentsÎncă nu există evaluări
- Spring Forest Qigong: With International Qigong Master Chunyi LinDocument43 paginiSpring Forest Qigong: With International Qigong Master Chunyi Linsparks91% (23)
- Tattooing The Body, Marking CultureDocument15 paginiTattooing The Body, Marking CultureLiliana AndreeaÎncă nu există evaluări
- Medical and Allied Health ProfessionDocument30 paginiMedical and Allied Health ProfessionAnalyn QueroÎncă nu există evaluări
- Community Based Surveillance Training ManualDocument48 paginiCommunity Based Surveillance Training ManualDana_niaÎncă nu există evaluări
- St. Stephen's Hospital: Dept of Endocrinology, Diabetes & Metabolic MedicineDocument6 paginiSt. Stephen's Hospital: Dept of Endocrinology, Diabetes & Metabolic MedicineDr ratna kumariÎncă nu există evaluări
- Measure Glucose 1977Document4 paginiMeasure Glucose 1977iprintÎncă nu există evaluări
- Class X HalfyearlyDocument5 paginiClass X HalfyearlySunil rathiÎncă nu există evaluări
- ACross CulturalTestoftheTraumaModelofDissociation2Document24 paginiACross CulturalTestoftheTraumaModelofDissociation2Fulop NoemiÎncă nu există evaluări