DOI: 10.5958/j.2319-5886.3.2.
100
International Journal of Medical Research & Health Sciences
www.ijmrhs.com Volume 3 Issue 2 (April - Jun) Coden: IJMRHS th Received: 25 Jan 2014 Revised: 20th Feb 2014
Case report
Copyright @2014 ISSN: 2319-5886 Accepted: 23rd Feb 2014
LEPTOSPIROSIS COMPLICATED WITH MENINGOENCEPHALITIS AND PANCREATITIS - A CASE REPORT *Sumantro Mondal1, Tony Ete1, Debanjali Sinha1, Soumik Sarkar1, Atanu Chakraborty1, Arijit Nag1, Jyotirmoy Pal2, Alakendu Ghosh3
1
Post graduate trainee, 2Associate Professor, 3Professor, Department of Medicine, Institute of Post Graduate Medical Education And Research, Kolkata, India *Corresponding author email: drmsumantro@gmail.com ABSTRACT In severe leptospirosis multi organ involvement is common. Pancreatitis and meningo encephalitis are two uncommon manifestations of leptospirosis. Our patient presented with fever, jaundice, altered sensorium and subsequently developed severe pain abdomen. He was finally diagnosed as having icteic leptospirosis complicated with pancreatitis and meningoencephalitis. Simultaneous presence of these two complications in a patient of leptospirosis probably not been documented before. Key words: Leptospirosis, Pancreatitis, Meningo encephalitis. INTRODUCTION Leptospirosis is a zoonosis, and is considered as a major public health problem. The clinical phenotypes of leptospirosis are diverse, ranging from mild, flulike illness to a severe disease form known as Weils syndrome. Severe disease is characterized by hepatic, renal and pulmonary involvement, which can lead to death. The disease may also present with some uncommon manifestations. Ascending progressive leg weakness, acalculous cholecystitis, hemorrhagic pneumonitis have been documented as atypical manifestations of leptospirosis in various literatures.1,2,3 Pancreatitis and meningoencephalitis are uncommon manifestations of leptospirosis. There are few case reports concerning leptospirosis complicated with either pancreatitis or meningoencephalitis. However presence of both pancreatitis and meningoencephalitis in a patient of leptospirosis is extremely rare. The case reported herein describes the concomitant presence of pancreatitis and meningoencephalitis in a patient of complicated leptospirosis. CASE REPORT A 32 year male, admitted with a history of moderate grade, intermittent fever for 10 days associated with mild cough. Fever was associated with redness of eyes and pain in muscles, especially calf regions. The patient developed yellowish discolouration of sclera 3 days prior to admission, repeated vomiting, drowsiness and diminution of urine volume since last 1 day. On the day of admission the patient developed intense pain in his upper abdomen. There was no history of any rash or convulsion. Examination revealed a confused patient (Glasgow coma scale: 11), severe pallor, icterus, neck rigidity, positive kernigs sign, pulse rate 114/minute and a blood pressure of 112/74 mm of Hg. Abdominal examination was inconclusive apart from sluggish peristaltic sound and hepatic enlargement. Other 477 Sumantro et al., Int J Med Res Health Sci. 2014;3(2):477-479
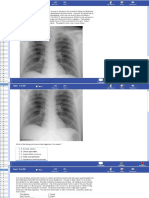
systems were normal. Routine blood investigations showed anemia (Hb 9.4GM/dl) with leucocytosis (15600/ cu.mm.) with neutrophilic predominance. Liver function was dearranged with a total bilirubin 11.7 mg/dl (conjugated 7.6 and unconjugated 4.1 mg/dl), SGOT 168 IU/L and SGPT 71 IU/L. Prothrombin time was normal. Serum urea 110 mg/dl, creatinine 4.1 mg/dl. CSF study showed cell count 36/cu.mm (70% lymphocyte), protein 76 mg/dl and sugar 48 mg/dl. CSF for Herpes simplex virus (HSV) and arbovirus were negative. Serum amylase (750 U/L) and lipase (3720 U/L) were elevated. CT scan of abdomen showed bulky pancreas with peri pancreatic fat stranding, suggestive of acute pancreatitis (Figure 1). Test for malaria parasite, vivax and falciperum antigen and IgM antibody for dengue were also negative. As there was a high index of suspicion of leptospirosis in this clinical setting serum Creatine phosphokinase (CPK) was sent and the value was 968 U/L (normal: 52-336 U/L). Later on leptospirosis was confirmed by a positive IgM anti leptospira antibody. The patient was treated with injection Ceftriaxone (1 GM/day i.v BD) and showed good clinical improvement over next 10 days. Follow up after 1 month showed normalization of liver function test parameters, CPK value with a normal CT scan of abdomen.
Fig 1: CT scan of abdomen at the level of pancreas showing bulky pancreas with mild peri pancreatic fat stranding suggestive of acute pancreatitis.
DISCUSSION Leptospirosis is a zoonoses and this disease entity is frequently found in India. The first recognized leptospiral disease was described by Weil in 1886. Causative agent of Weils disease was isolated in 1915 and named Leptospira icterohaemorrhagiae. Leptospirosis has two clinically recognizable Sumantro et al.,
phenotype the anicteric leptospirosis (80-90% of all cases) and icteric leptospirosis. Apart from hepatic and renal involvement, various other organs are frequently affected in leptospirosis. Pancreatitis is an unusual manifestation of leptospirosis affecting approximately 25% of patients. There are some case reports regarding pancreatitis in leptospirosis.4,5 In our patient pancreatitis was confirmed by both laboratory investigation and imaging and there was no other common cause of pancreatitis like gall stone, alcoholism or drug intake. Though the exact mechanism of acute pancreatitis in leptospirosis has not been clearly established, vasculitis of small vessels with ischemic injury leading to activation of proteolytic enzymes and pancreatic auto-digestion is the possible mechanism.6 Features of meningo encephalitis, as seen in our patient are also uncommon in leptospirosis. Currently there are not enough published data about neurological features in Leptospirosis. In one study it was found that only 5.9% patient can present with signs of meningism. 7 Another prospective study conducted in France among 62 cases of leptospirosis meningo encephalitis was documented in only 2 patients, signifying rarity of this feature. 8 In a study by Matiash VI, et al. on 120 patients with fatal icterohemorrhagic leptospirosis, neurotoxicosis was evident in almost all patients along with microcirculatory disturbances. Meningitis was found in 29.2%, meningoencephalitis in 5% of patients. Morphologic studies showed that focal serous meningitides and meningoencephalitides were significantly more common that they are diagnosed in clinical settings. They tend to develop during the second and third weeks of the course of the illness.9 Seizures and altered sensorium are most common neurological manifestation of leptospirosis.10 Alteration of sensorium and signs of meningeal irritation were present in our patient along with lymphocytic pleocytosis in CSF study, establishing a diagnosis of meningoencephalitis. Concomitant presence of encephalitis and pancreatitis in a patient with leptospirosis is very rare and probably not reported before. It should be emphasized that neuroleptospirosis is an important differential diagnosis of cerebral malaria, dengue and other viral encephalitis, especially in the Indian subcontinent.
478 Int J Med Res Health Sci. 2014;3(2):477-479
REFERENCES 1. Silva AP, Burg LB, Locatelli JF, Manes J, Crispim M. Leptospirosis presenting as ascending progressive leg weakness and complicating with acute pancreatitis. Braz J Infect Dis. 2011; 15(5): 493-97 2. Peter G, Narasimha H. Acalculous cholecystitis: a rare presentation ofleptospirosis progressing to Weil's disease. Asian Pac J Trop Med. 2011;4(12):1007-08 3. Pai ND, Adhikari PM. Haemorrhagic pneumonitis: A rare presentation of leptospirosis. J Postgrad Med. 2001;47(1):35-36 4. Baburaj P, Antony T, Louis F, Harikrishnan BL. Acute abdomen due to acute pancreatitis--a rare presentation of leptospirosis. J Assoc Physicians India. 2008; 56:911-12 5. Kaya E, Dervisoglu A, Eroglu C, Polat C, Sunbul M, Ozkan K. Acute pancreatitiscaused by leptospirosis: report of two cases. World J Gastroenterol. 2005; 11(28):4447-49 6. A Desai, D Hattanga. Leptospirosis As A Rare Cause Of Acute Pancreatitis. The internet journal of surgery. 2008;20(1):DOI 7. Datta S, Sarkar RN, Biswas A, Mitra S. Leptospirosis: an institutional experience. J Indian Med Assoc. 2011; 109(10):737-78 8. Abgueguen P, Delbos V, Blanvillain J, Chennebault JM, Cottin J, Fanello S, et al. Clinical aspects and prognostic factors of leptospirosis in adults. Retrospective study in France. J Infect. 2008;57(3):171-78 9. Matiash VI, Anisimova IuN. The clinicomorphological characteristics of the nervous system lesions in icterohemorrhagic leptospirosis. Lik Sprava. 1997;( 3):94-99 10. Mathew T, Satishchandra P, Mahadevan A, Nagarathna S, Yasha TC, Chandramukhi A, et al. Neuroleptospirosis-revisited: experience from a tertiary care neurological centre from south India. Indian J Med Res 2006; 124: 155-62.
479 Sumantro et al., Int J Med Res Health Sci. 2014;3(2):477-479
S-ar putea să vă placă și
- Leptospirosis CasosDocument2 paginiLeptospirosis CasosfelipeÎncă nu există evaluări
- 51 Uysal EtalDocument4 pagini51 Uysal EtaleditorijmrhsÎncă nu există evaluări
- 68 JMSCRDocument3 pagini68 JMSCRVani Junior LoverzÎncă nu există evaluări
- Acute Fulminant Leptospirosis with Multi-Organ FailureDocument4 paginiAcute Fulminant Leptospirosis with Multi-Organ FailureMuhFarizaAudiÎncă nu există evaluări
- A Case of Lupus Pneumonitis Mimicking As Infective PneumoniaDocument4 paginiA Case of Lupus Pneumonitis Mimicking As Infective PneumoniaIOSR Journal of PharmacyÎncă nu există evaluări
- Acute Appendicitis in A Patient With Systemic Lupus ErythematosusDocument4 paginiAcute Appendicitis in A Patient With Systemic Lupus ErythematosusJessicaÎncă nu există evaluări
- Jeyasuriya Et AlDocument3 paginiJeyasuriya Et AlInternational Journal of Clinical and Biomedical Research (IJCBR)Încă nu există evaluări
- Acute Surgical Abdomen: Unexpected Medical CauseDocument6 paginiAcute Surgical Abdomen: Unexpected Medical CauseIJAR JOURNALÎncă nu există evaluări
- A Case Report On Potts Spine Spinal TubeDocument3 paginiA Case Report On Potts Spine Spinal TubeyaneemayÎncă nu există evaluări
- Case 1Document4 paginiCase 1Irsanti SasmitaÎncă nu există evaluări
- Seronegative Myasthenia Gravis Presenting With PneumoniaDocument4 paginiSeronegative Myasthenia Gravis Presenting With PneumoniaJ. Ruben HermannÎncă nu există evaluări
- Typhoid Fever Case Presenting with Multiple ComplicationsDocument4 paginiTyphoid Fever Case Presenting with Multiple ComplicationsCleo CaminadeÎncă nu există evaluări
- Pan 1Document3 paginiPan 1Mithun CbÎncă nu există evaluări
- Severe Acute Pancreatitis - A Serious Complication of LeptospirosisDocument3 paginiSevere Acute Pancreatitis - A Serious Complication of LeptospirosisSanda Puspa RiniÎncă nu există evaluări
- Leptospirosis: A Case Study: Mathew SullivanDocument3 paginiLeptospirosis: A Case Study: Mathew SullivanSagara MaheshÎncă nu există evaluări
- ISCA-IRJMedS-2014-058Document3 paginiISCA-IRJMedS-2014-058KarenÎncă nu există evaluări
- BMC Dermatology: Schönlein-Henoch Purpura During Pregnancy With Successful Outcome For Mother and NewbornDocument5 paginiBMC Dermatology: Schönlein-Henoch Purpura During Pregnancy With Successful Outcome For Mother and NewbornteguhÎncă nu există evaluări
- Iaet 12 I 2 P 135Document2 paginiIaet 12 I 2 P 135leonjunchan_66965707Încă nu există evaluări
- Al12 1 JuvenileDocument24 paginiAl12 1 JuvenileDiego Alberto Hernández CatalánÎncă nu există evaluări
- A Rare Cause of Endocarditis: Streptococcus PyogenesDocument3 paginiA Rare Cause of Endocarditis: Streptococcus PyogenesYusuf BrilliantÎncă nu există evaluări
- LeptospirosisDocument6 paginiLeptospirosiskadek angga ari darmawanÎncă nu există evaluări
- Experimental Evidence of Obesity As A Risk Factor For Severe Acute PancreatitisDocument6 paginiExperimental Evidence of Obesity As A Risk Factor For Severe Acute Pancreatitisnugroho akhbarÎncă nu există evaluări
- Ijss Nov cr08 PDFDocument3 paginiIjss Nov cr08 PDFRoyÎncă nu există evaluări
- Soldiers From Indo Myanmar Border Presenting With Scrub Typhus: Case ReportDocument5 paginiSoldiers From Indo Myanmar Border Presenting With Scrub Typhus: Case ReportIOSRjournalÎncă nu există evaluări
- Abdominal Pain As A Presenting Feature in Malaria: Sri Lanka Journal of Child Health, 2010 39: 158-159Document2 paginiAbdominal Pain As A Presenting Feature in Malaria: Sri Lanka Journal of Child Health, 2010 39: 158-159Shalina AbalosÎncă nu există evaluări
- Intestinal Tuberculosis: A Diagnostic Challenge: Open Access Case DOI: 10.7759/cureus.13058Document4 paginiIntestinal Tuberculosis: A Diagnostic Challenge: Open Access Case DOI: 10.7759/cureus.13058ATIKA INDAH SARIÎncă nu există evaluări
- Hyperacute Liver Failure With Multi-Organ Dysfunction Syndrome (MODS) by Leptospirosis: A Case ReportDocument3 paginiHyperacute Liver Failure With Multi-Organ Dysfunction Syndrome (MODS) by Leptospirosis: A Case ReportMinerva Medical Treatment Pvt LtdÎncă nu există evaluări
- 56 SyedDocument3 pagini56 SyededitorijmrhsÎncă nu există evaluări
- Short-Term Outcome of Proliferative Lupus Nephritis A Single Center StudyDocument12 paginiShort-Term Outcome of Proliferative Lupus Nephritis A Single Center StudyTJPRC PublicationsÎncă nu există evaluări
- Treatment of Refractory Pyoderma Gangrenosum with Infliximab in a 17-Month-Old BoyDocument6 paginiTreatment of Refractory Pyoderma Gangrenosum with Infliximab in a 17-Month-Old BoyJares Clinton Saragih SimarmataÎncă nu există evaluări
- Jurnal AppendiksDocument6 paginiJurnal AppendiksSiti anasya CahyaÎncă nu există evaluări
- Pathologic Quiz Case: Residents' PageDocument4 paginiPathologic Quiz Case: Residents' Pagejeka222Încă nu există evaluări
- PTU-Induced Vasculitis in a Teen with HyperthyroidismDocument4 paginiPTU-Induced Vasculitis in a Teen with HyperthyroidismGene LlanoraÎncă nu există evaluări
- Early Relapse Could Predict Unfavorable Prognosis in Nephrotic SyndromeDocument6 paginiEarly Relapse Could Predict Unfavorable Prognosis in Nephrotic SyndromeBianti Nur'ainiÎncă nu există evaluări
- Pediatric Systemic Lupus Erythematosus Associated With AutoimmuneDocument9 paginiPediatric Systemic Lupus Erythematosus Associated With AutoimmunegistaluvikaÎncă nu există evaluări
- 54 Shivraj EtalDocument3 pagini54 Shivraj EtaleditorijmrhsÎncă nu există evaluări
- JCIMCR v3 1706Document2 paginiJCIMCR v3 1706Mohan ChikkalaÎncă nu există evaluări
- Paraplegia in Dengue PatientDocument3 paginiParaplegia in Dengue PatientAshwaq TpÎncă nu există evaluări
- 85 JMSCRDocument3 pagini85 JMSCRVani Junior LoverzÎncă nu există evaluări
- Potts DiseaseDocument6 paginiPotts DiseaseJefferson ManasanÎncă nu există evaluări
- LepsDocument4 paginiLepslynharee100% (1)
- Understanding Lupus NephritisDocument21 paginiUnderstanding Lupus Nephritissaritha Oruganti100% (1)
- Images For Surgeons: Abdominal Tuberculosis: An Easily Forgotten DiagnosisDocument2 paginiImages For Surgeons: Abdominal Tuberculosis: An Easily Forgotten DiagnosisRisti Khafidah100% (1)
- Delay in Diagnosis of Extra-Pulmonary Tuberculosis by Its Rare Manifestations: A Case ReportDocument5 paginiDelay in Diagnosis of Extra-Pulmonary Tuberculosis by Its Rare Manifestations: A Case ReportSneeze LouderÎncă nu există evaluări
- Mistaken Identity Reporting Two Cases of Rare Fo 2024 International JournalDocument7 paginiMistaken Identity Reporting Two Cases of Rare Fo 2024 International JournalRonald QuezadaÎncă nu există evaluări
- Rare Spinal InfectionDocument3 paginiRare Spinal InfectionAlam MartadipuraÎncă nu există evaluări
- Unusual Case of Tuberculous Pleural Effusion and Abdominal MassDocument4 paginiUnusual Case of Tuberculous Pleural Effusion and Abdominal MassRofi IrmanÎncă nu există evaluări
- Acute Pyelonephritis in Adults: A Case Series of 223 PatientsDocument6 paginiAcute Pyelonephritis in Adults: A Case Series of 223 PatientsshiaÎncă nu există evaluări
- Pancytopenia Secondary To Bacterial SepsisDocument16 paginiPancytopenia Secondary To Bacterial Sepsisiamralph89Încă nu există evaluări
- Case Report: Peritonitis in Patients With Scrub TyphusDocument3 paginiCase Report: Peritonitis in Patients With Scrub TyphusJasleen KaurÎncă nu există evaluări
- Pleural Effusion in A Patient With End-Stage Renal Disease - PMCDocument5 paginiPleural Effusion in A Patient With End-Stage Renal Disease - PMCCasemix rsudwaledÎncă nu există evaluări
- Case Report On Bilateral Emphysematous Pyelonephr - 2024 - International JournalDocument4 paginiCase Report On Bilateral Emphysematous Pyelonephr - 2024 - International JournalRonald QuezadaÎncă nu există evaluări
- Abdominal Tuberculosis in Nepal Medical College Teaching Hospital, KathmanduDocument4 paginiAbdominal Tuberculosis in Nepal Medical College Teaching Hospital, KathmanduSavitri Maharani BudimanÎncă nu există evaluări
- Poliadenitis NodosaDocument5 paginiPoliadenitis NodosaRicardo Uzcategui ArreguiÎncă nu există evaluări
- Prophylaxis Against Fungal Peritonitis in CAPD A Single Center Experience With Low Dose FluconazoleDocument5 paginiProphylaxis Against Fungal Peritonitis in CAPD A Single Center Experience With Low Dose FluconazoleJorge David Gamez PeñarandaÎncă nu există evaluări
- Respiratory and Pulmonary Medicine: ClinmedDocument3 paginiRespiratory and Pulmonary Medicine: ClinmedGrace Yuni Soesanti MhÎncă nu există evaluări
- The Importance of Genetic Testing in Adolescent-Onset Steroid-Resistant Nephrotic Syndrome - Case ReportDocument9 paginiThe Importance of Genetic Testing in Adolescent-Onset Steroid-Resistant Nephrotic Syndrome - Case ReportAlrista MawarÎncă nu există evaluări
- Isolated Thrombocytopenia A Rare Presenting Feature of Enteric FeverDocument2 paginiIsolated Thrombocytopenia A Rare Presenting Feature of Enteric FeverputiridhaÎncă nu există evaluări
- Eosinophilic Granulomatosis With Polyangiitis and Bowel Perforation: Case ReportDocument5 paginiEosinophilic Granulomatosis With Polyangiitis and Bowel Perforation: Case ReportSabrina JonesÎncă nu există evaluări
- Diagnosis and Treatment of Chronic CoughDe la EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoÎncă nu există evaluări
- Ijmrhs Vol 3 Issue 1Document228 paginiIjmrhs Vol 3 Issue 1editorijmrhsÎncă nu există evaluări
- Ijmrhs Vol 4 Issue 3Document263 paginiIjmrhs Vol 4 Issue 3editorijmrhsÎncă nu există evaluări
- Ijmrhs Vol 4 Issue 2Document219 paginiIjmrhs Vol 4 Issue 2editorijmrhsÎncă nu există evaluări
- Ijmrhs Vol 4 Issue 4Document193 paginiIjmrhs Vol 4 Issue 4editorijmrhs0% (1)
- Ijmrhs Vol 1 Issue 1Document257 paginiIjmrhs Vol 1 Issue 1editorijmrhsÎncă nu există evaluări
- Ijmrhs Vol 2 Issue 4Document321 paginiIjmrhs Vol 2 Issue 4editorijmrhsÎncă nu există evaluări
- Ijmrhs Vol 3 Issue 2Document281 paginiIjmrhs Vol 3 Issue 2editorijmrhsÎncă nu există evaluări
- Ijmrhs Vol 3 Issue 4Document294 paginiIjmrhs Vol 3 Issue 4editorijmrhsÎncă nu există evaluări
- Ijmrhs Vol 3 Issue 3Document271 paginiIjmrhs Vol 3 Issue 3editorijmrhsÎncă nu există evaluări
- 45mohit EtalDocument4 pagini45mohit EtaleditorijmrhsÎncă nu există evaluări
- Ijmrhs Vol 2 Issue 3Document399 paginiIjmrhs Vol 2 Issue 3editorijmrhs100% (1)
- Ijmrhs Vol 2 Issue 2Document197 paginiIjmrhs Vol 2 Issue 2editorijmrhsÎncă nu există evaluări
- Ijmrhs Vol 2 Issue 1Document110 paginiIjmrhs Vol 2 Issue 1editorijmrhs100% (1)
- Ijmrhs Vol 1 Issue 1Document257 paginiIjmrhs Vol 1 Issue 1editorijmrhsÎncă nu există evaluări
- 47serban Turliuc EtalDocument4 pagini47serban Turliuc EtaleditorijmrhsÎncă nu există evaluări
- 48 MakrandDocument2 pagini48 MakrandeditorijmrhsÎncă nu există evaluări
- 36rashmipal EtalDocument6 pagini36rashmipal EtaleditorijmrhsÎncă nu există evaluări
- Recurrent Cornual Ectopic Pregnancy - A Case Report: Article InfoDocument2 paginiRecurrent Cornual Ectopic Pregnancy - A Case Report: Article InfoeditorijmrhsÎncă nu există evaluări
- 41anurag EtalDocument2 pagini41anurag EtaleditorijmrhsÎncă nu există evaluări
- Williams-Campbell Syndrome-A Rare Entity of Congenital Bronchiectasis: A Case Report in AdultDocument3 paginiWilliams-Campbell Syndrome-A Rare Entity of Congenital Bronchiectasis: A Case Report in AdulteditorijmrhsÎncă nu există evaluări
- 43chaitali EtalDocument3 pagini43chaitali EtaleditorijmrhsÎncă nu există evaluări
- 38vaishnavi EtalDocument3 pagini38vaishnavi EtaleditorijmrhsÎncă nu există evaluări
- 40vedant EtalDocument4 pagini40vedant EtaleditorijmrhsÎncă nu există evaluări
- 37poflee EtalDocument3 pagini37poflee EtaleditorijmrhsÎncă nu există evaluări
- 35krishnasamy EtalDocument1 pagină35krishnasamy EtaleditorijmrhsÎncă nu există evaluări
- Pernicious Anemia in Young: A Case Report With Review of LiteratureDocument5 paginiPernicious Anemia in Young: A Case Report With Review of LiteratureeditorijmrhsÎncă nu există evaluări
- 34tupe EtalDocument5 pagini34tupe EtaleditorijmrhsÎncă nu există evaluări
- 32bheemprasad EtalDocument3 pagini32bheemprasad EtaleditorijmrhsÎncă nu există evaluări
- 33 Prabu RamDocument5 pagini33 Prabu RameditorijmrhsÎncă nu există evaluări
- Council 2016 AnswerDocument44 paginiCouncil 2016 AnsweralicÎncă nu există evaluări
- Cholecystitis: What Is It?Document6 paginiCholecystitis: What Is It?Aziil LiizaÎncă nu există evaluări
- Liver, Pancreas and Biliary Tract Problems: Case StudyDocument62 paginiLiver, Pancreas and Biliary Tract Problems: Case StudyElaine Frances IlloÎncă nu există evaluări
- 13 common digestive diseasesDocument8 pagini13 common digestive diseasesBulcio Reed NaxilaÎncă nu există evaluări
- Marolf2012 US Colangite FelinosDocument7 paginiMarolf2012 US Colangite FelinosThaís ChouinÎncă nu există evaluări
- Gastrointestinal ImagingDocument134 paginiGastrointestinal ImagingAnonymous RTSL19BmiÎncă nu există evaluări
- (The Clinics - Surgery) Steve Behrman MD FACS, Ron Martin MD FACS - Modern Concepts in Pancreatic Surgery, An Issue of Surgical Clinics, 1e (2013, Elsevier)Document197 pagini(The Clinics - Surgery) Steve Behrman MD FACS, Ron Martin MD FACS - Modern Concepts in Pancreatic Surgery, An Issue of Surgical Clinics, 1e (2013, Elsevier)Yee Wei HoongÎncă nu există evaluări
- Pancreatitis Aguda: Erik Rauch Sánchez Médico Gastroenterólogo Febrero 2016. / 999 290 697Document30 paginiPancreatitis Aguda: Erik Rauch Sánchez Médico Gastroenterólogo Febrero 2016. / 999 290 697NickÎncă nu există evaluări
- Shackelford S Surgery of The Alimentary Tract Yeo 8 Ed 2019Document2.400 paginiShackelford S Surgery of The Alimentary Tract Yeo 8 Ed 2019Shuler007193% (29)
- Development of FUJI DRI-CHEM v-LIP-P Slide that Achieves High Specificity for Measuring Canine and Feline Pancreatic LipaseDocument7 paginiDevelopment of FUJI DRI-CHEM v-LIP-P Slide that Achieves High Specificity for Measuring Canine and Feline Pancreatic LipaseAngelesÎncă nu există evaluări
- Gastric and Intestinal DisorderDocument13 paginiGastric and Intestinal DisorderMei Joy100% (1)
- Case Report of Acute Biliary PancreatitisDocument12 paginiCase Report of Acute Biliary Pancreatitisfiareza dilagaÎncă nu există evaluări
- Causes of Acute Abdominal Pain in Children and Adolescents - UpToDateDocument22 paginiCauses of Acute Abdominal Pain in Children and Adolescents - UpToDateJéssica SantosÎncă nu există evaluări
- Usmle Step 2 CK Recalls 2021 3jz DR NotesDocument22 paginiUsmle Step 2 CK Recalls 2021 3jz DR Notesmed student100% (2)
- Procedure List With AmountDocument20 paginiProcedure List With AmountMadhavan MadeshsanthoshÎncă nu există evaluări
- Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDocument4 paginiPractice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralÎncă nu există evaluări
- Pancretits Aguda No ComplicadaDocument14 paginiPancretits Aguda No Complicadaaroldoe99Încă nu există evaluări
- Üds 2008 Sağlık Sonbahar EkimDocument15 paginiÜds 2008 Sağlık Sonbahar EkimDr. Hikmet ŞahinerÎncă nu există evaluări
- Acute Pancreatitis Case PresDocument29 paginiAcute Pancreatitis Case Preskristine keen buanÎncă nu există evaluări
- NCLEX Practice Questions - Digestive System 3Document11 paginiNCLEX Practice Questions - Digestive System 3Geevee Naganag VentulaÎncă nu există evaluări
- NAVLE - ReviewsDocument3 paginiNAVLE - ReviewsEvaldo Mamedes0% (1)
- Gastrointestinal & NutritionBlock2 PDFDocument183 paginiGastrointestinal & NutritionBlock2 PDFTed DoyleÎncă nu există evaluări
- Studi KasusDocument3 paginiStudi KasusJulian FelixÎncă nu există evaluări
- Video Recap of Enzymes by Amoeba SistersDocument2 paginiVideo Recap of Enzymes by Amoeba Sistersapi-2331875660% (1)
- Nutrition in The Critically Ill PatientDocument13 paginiNutrition in The Critically Ill PatientnainazahraÎncă nu există evaluări
- Acute PancreatitisDocument2 paginiAcute PancreatitisPrincess Aliha M. JIMENEZÎncă nu există evaluări
- Hughes Necrotizing PancreatitisDocument11 paginiHughes Necrotizing PancreatitisELizabeth OlmosÎncă nu există evaluări
- SCORES and CRITERIAS For Last Minute by DR RRMDocument52 paginiSCORES and CRITERIAS For Last Minute by DR RRMShweta Achuthan KuttyÎncă nu există evaluări
- BioDocument2 paginiBioRana bilalÎncă nu există evaluări
- A19321120ap31134106 RLSDocument29 paginiA19321120ap31134106 RLSSukanya SubramanianÎncă nu există evaluări