S-ar putea să vă placă și
- DAVIS MedSurg Notes Nurse S Clinical Pocket Guide FA Davis 2007Document242 paginiDAVIS MedSurg Notes Nurse S Clinical Pocket Guide FA Davis 2007amaliea234100% (1)
- Genetic DiseasesDocument108 paginiGenetic DiseasesRizki Widya NurÎncă nu există evaluări
- Early Theories of Cancer PDFDocument16 paginiEarly Theories of Cancer PDFLiza Marie Cayetano AdarneÎncă nu există evaluări
- GERIATRIC MEDICINE Lecture (Original)Document35 paginiGERIATRIC MEDICINE Lecture (Original)Dwi Wulandari100% (1)
- TB TreatmentDocument58 paginiTB TreatmentNdayisaba CorneilleÎncă nu există evaluări
- 2007 Menstrual History QuestionnaireDocument2 pagini2007 Menstrual History QuestionnaireAnonymous kieXEbsGeÎncă nu există evaluări
- Real Exam Ethics OSCEDocument3 paginiReal Exam Ethics OSCEmonica ortizÎncă nu există evaluări
- Chart FastingDocument1 paginăChart FastingGary S75% (4)
- Lewis CH 42 GIDocument13 paginiLewis CH 42 GIwismommyÎncă nu există evaluări
- Health Information Form: For AdultsDocument15 paginiHealth Information Form: For AdultsDavid KingÎncă nu există evaluări
- 1 - Elzohry MasterClass 2010 (MRCP Part2)Document839 pagini1 - Elzohry MasterClass 2010 (MRCP Part2)tejbirsingh2013100% (4)
- Diarrhoea Guidelines PDFDocument58 paginiDiarrhoea Guidelines PDFmustikaarumÎncă nu există evaluări
- Metronidazole Drug StudyDocument2 paginiMetronidazole Drug StudyJessica Christine Datuin Gustilo100% (1)
- Clinical training guide for ERPM candidatesDocument33 paginiClinical training guide for ERPM candidatesAmal Perera100% (1)
- Metronidazole Baxter in FDocument12 paginiMetronidazole Baxter in Fgautam gurjarÎncă nu există evaluări
- Metronidazole AFTinfDocument8 paginiMetronidazole AFTinfSmartishag BediakoÎncă nu există evaluări
- Metronidazole Injection for Treating Anaerobic Bacterial InfectionsDocument20 paginiMetronidazole Injection for Treating Anaerobic Bacterial InfectionsYuniÎncă nu există evaluări
- Dailymed - Nlm.nih - Gov METRONIDAZOLEDocument16 paginiDailymed - Nlm.nih - Gov METRONIDAZOLELip StickÎncă nu există evaluări
- Clinical Pharmacology Module 14 1Document14 paginiClinical Pharmacology Module 14 1Steven Mark MananguÎncă nu există evaluări
- Klint Klint: Tablets/Injection SuspensionDocument1 paginăKlint Klint: Tablets/Injection SuspensionibtesamÎncă nu există evaluări
- Flagyl Metronidazole TabletsDocument11 paginiFlagyl Metronidazole TabletsYantari TiyoraÎncă nu există evaluări
- FlagystatinDocument18 paginiFlagystatinChristian YongkyÎncă nu există evaluări
- Flagyl-suspension-SmPC-05.2021 For DistributionDocument9 paginiFlagyl-suspension-SmPC-05.2021 For Distributionrx bafnaÎncă nu există evaluări
- MetronidazoleDocument3 paginiMetronidazoleAvigale Arcillas BasilioÎncă nu există evaluări
- Metronidazole Problems and Solutions ReviewDocument21 paginiMetronidazole Problems and Solutions Reviewصباح جوادÎncă nu există evaluări
- Preformulation of MetronidazoleDocument11 paginiPreformulation of MetronidazoleJoseLuisHuamanÎncă nu există evaluări
- Metronidazol PropiedadesDocument9 paginiMetronidazol PropiedadesYonatan Gómez VargasÎncă nu există evaluări
- Anti-Amoebic Drugs: Madan Sigdel Lecturer Department of Pharmacology Gandaki Medical CollegeDocument21 paginiAnti-Amoebic Drugs: Madan Sigdel Lecturer Department of Pharmacology Gandaki Medical Collegemadan sigdelÎncă nu există evaluări
- Metro Dinaz OleDocument3 paginiMetro Dinaz OleFadli ArchieÎncă nu există evaluări
- Metro Nida ZolDocument9 paginiMetro Nida ZolAnna Thalita CardosoÎncă nu există evaluări
- MetronidazoleDocument5 paginiMetronidazoleGwyneth JangadÎncă nu există evaluări
- Metoclopramide HCL Metoclopramide Inj 10mg-2ml IreDocument7 paginiMetoclopramide HCL Metoclopramide Inj 10mg-2ml IresiripÎncă nu există evaluări
- Anthelmintic Drugs: Pharmacology IvDocument27 paginiAnthelmintic Drugs: Pharmacology IvShashidharan MenonÎncă nu există evaluări
- Flagystatin SG 1222Document15 paginiFlagystatin SG 1222MarjMalubayArriolaÎncă nu există evaluări
- Dexamethasone Sodium PhosphateDocument14 paginiDexamethasone Sodium PhosphateYunita WidyaningsihÎncă nu există evaluări
- Depo MedrolDocument33 paginiDepo MedrolarianjafarirmÎncă nu există evaluări
- Obat - BMDocument50 paginiObat - BMNovita PermataÎncă nu există evaluări
- Baby Case Study (FINAL)Document44 paginiBaby Case Study (FINAL)Rouie Björn ABrianÎncă nu există evaluări
- Therapeutic Uses of Metronidazole and Its Side Effects: An UpdateDocument5 paginiTherapeutic Uses of Metronidazole and Its Side Effects: An UpdateSandrina NajwaÎncă nu există evaluări
- Medsafe Data Sheet Dotareminj - Prefilled Syringe PDFDocument6 paginiMedsafe Data Sheet Dotareminj - Prefilled Syringe PDFizalxrayÎncă nu există evaluări
- Tinidazole Is An AntiDocument6 paginiTinidazole Is An AntiNoi Maya Anggrita SariÎncă nu există evaluări
- Decadron: (Dexamethasone Tablets, Usp)Document8 paginiDecadron: (Dexamethasone Tablets, Usp)Anonymous QqyLDoW1Încă nu există evaluări
- (500 MG Metronidazole and 100,000 IU Nystatin) Vaginal OvulesDocument22 pagini(500 MG Metronidazole and 100,000 IU Nystatin) Vaginal OvulesAngel CoÎncă nu există evaluări
- C1C13 and C14-Methotrexate - Methotrexate Sodium (CPhA Monograph)Document13 paginiC1C13 and C14-Methotrexate - Methotrexate Sodium (CPhA Monograph)Mina AzmyÎncă nu există evaluări
- Antoprotozoal DrugsDocument29 paginiAntoprotozoal DrugsAdil MusaddiqÎncă nu există evaluări
- Farmakologi Obat Kusta Dan Antiparasit 2015Document84 paginiFarmakologi Obat Kusta Dan Antiparasit 2015Alex FerdinandÎncă nu există evaluări
- Metronidazole uses, side effects and nursing considerationsDocument2 paginiMetronidazole uses, side effects and nursing considerationshauteanicoleÎncă nu există evaluări
- 12623slr059 Flagyl LBLDocument7 pagini12623slr059 Flagyl LBLgeeenaaÎncă nu există evaluări
- Daunorubicin: Drug NameDocument7 paginiDaunorubicin: Drug NameEdgar Ledesma-MartínezÎncă nu există evaluări
- Trusopt: (Dorzolamide Hydrochloride Ophthalmic Solution)Document16 paginiTrusopt: (Dorzolamide Hydrochloride Ophthalmic Solution)Upik MoritaÎncă nu există evaluări
- EPS Ec MetoclopramideDocument3 paginiEPS Ec MetoclopramideMrprads5Încă nu există evaluări
- Mot Ilium TabDocument11 paginiMot Ilium TabChandra FatmaÎncă nu există evaluări
- S 039 LBLDocument45 paginiS 039 LBLAstha BhalodiaÎncă nu există evaluări
- Pharmacology Final Exam Name: SectionDocument19 paginiPharmacology Final Exam Name: SectionGlen Norwel LabayogÎncă nu există evaluări
- Keto Vs Mikonazol PharmacologyDocument6 paginiKeto Vs Mikonazol PharmacologyRanda NovalinoÎncă nu există evaluări
- KETOCONAZOLEDocument22 paginiKETOCONAZOLEAbdul khodir jaelaniÎncă nu există evaluări
- Ethambutol HydrochlorideDocument10 paginiEthambutol HydrochlorideAdithFullÎncă nu există evaluări
- MetronidazoleDocument26 paginiMetronidazoleNdayisaba CorneilleÎncă nu există evaluări
- Danladi Emmanuel 20CH1024Document11 paginiDanladi Emmanuel 20CH1024Mohammed kashimÎncă nu există evaluări
- AntimetabolitesDocument25 paginiAntimetabolitestheintrovÎncă nu există evaluări
- Nor Metrogyl KDocument5 paginiNor Metrogyl KManish ShankarpureÎncă nu există evaluări
- Antiprotozoal Drugs I: Metronidazole and Tinidazole for AmebiasisDocument36 paginiAntiprotozoal Drugs I: Metronidazole and Tinidazole for AmebiasisShashidharan MenonÎncă nu există evaluări
- ETHAMBUTOLDocument11 paginiETHAMBUTOLIrbasMantiniSyaifulÎncă nu există evaluări
- Nitrofurantoin: Tejal Khade Assistant Professor KGRDCP & RiDocument10 paginiNitrofurantoin: Tejal Khade Assistant Professor KGRDCP & RiAkshada bhangreÎncă nu există evaluări
- For Practitioner: Tuberculosis and Chronic Renal Failure Therapy PatternsDocument3 paginiFor Practitioner: Tuberculosis and Chronic Renal Failure Therapy PatternsAnastasia Lilian SuryajayaÎncă nu există evaluări
- Antiproto & AnthelminticsDocument57 paginiAntiproto & AnthelminticsDrMohan GuptaÎncă nu există evaluări
- RPHS 084Document8 paginiRPHS 084Amik IndrayaniÎncă nu există evaluări
- Medical Management 3 Objectives of ManagementDocument4 paginiMedical Management 3 Objectives of ManagementSaima Sawal SalicÎncă nu există evaluări
- Targocid - PI - Sanofi Aventis - MCC Format 24 January 2019Document15 paginiTargocid - PI - Sanofi Aventis - MCC Format 24 January 2019DR JAMAL WARISÎncă nu există evaluări
- The Essential Guide to Metronidazole: Usage, Precautions, Interactions and Side Effects.De la EverandThe Essential Guide to Metronidazole: Usage, Precautions, Interactions and Side Effects.Încă nu există evaluări
- NANOTECHNOLOGY REVIEW: LIPOSOMES, NANOTUBES & PLGA NANOPARTICLESDe la EverandNANOTECHNOLOGY REVIEW: LIPOSOMES, NANOTUBES & PLGA NANOPARTICLESÎncă nu există evaluări
- Gastric Volvulus: Bang Chau, Susan DufelDocument2 paginiGastric Volvulus: Bang Chau, Susan DufelmustikaarumÎncă nu există evaluări
- Nutrition and Stroke: Review ArticleDocument9 paginiNutrition and Stroke: Review Articlerichie_ciandraÎncă nu există evaluări
- 24 4 385Document6 pagini24 4 385mustikaarumÎncă nu există evaluări
- Dietary Fiber Intake in Early Pregnancy and Risk of Subsequent PreeclampsiaDocument7 paginiDietary Fiber Intake in Early Pregnancy and Risk of Subsequent PreeclampsiamustikaarumÎncă nu există evaluări
- Bushra, 2010Document7 paginiBushra, 2010Citta ArastiÎncă nu există evaluări
- Cooking RequirementsDocument1 paginăCooking RequirementsvectorÎncă nu există evaluări
- Logistics Execution Suite Manages Warehouse OperationsDocument9 paginiLogistics Execution Suite Manages Warehouse OperationsmustikaarumÎncă nu există evaluări
- ViaClinica RICA EnglishDocument127 paginiViaClinica RICA EnglishmustikaarumÎncă nu există evaluări
- Vitamind - TB PDFDocument7 paginiVitamind - TB PDFmustikaarumÎncă nu există evaluări
- Parenteral Nutrition in Critical CareDocument5 paginiParenteral Nutrition in Critical CaremustikaarumÎncă nu există evaluări
- Tingkat Pengetahuan Dan Praktik Penjamah Makanan Tentang Keamanan Pangan Pada Usaha Katering Di Kota MakassarDocument4 paginiTingkat Pengetahuan Dan Praktik Penjamah Makanan Tentang Keamanan Pangan Pada Usaha Katering Di Kota MakassarmustikaarumÎncă nu există evaluări
- Selected Health IndicatorsDocument93 paginiSelected Health IndicatorsmustikaarumÎncă nu există evaluări
- Nutrition Management - Sirosis PDFDocument10 paginiNutrition Management - Sirosis PDFmustikaarumÎncă nu există evaluări
- Nutrition Management - Sirosis PDFDocument10 paginiNutrition Management - Sirosis PDFmustikaarumÎncă nu există evaluări
- Nutrition Management - Sirosis PDFDocument10 paginiNutrition Management - Sirosis PDFmustikaarumÎncă nu există evaluări
- Laporan Week 9 BDocument36 paginiLaporan Week 9 BmustikaarumÎncă nu există evaluări
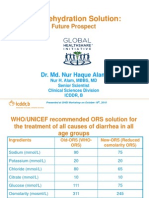
- Oral Rehydration Solution:: Future ProspectDocument48 paginiOral Rehydration Solution:: Future ProspectmustikaarumÎncă nu există evaluări
- BCAADocument8 paginiBCAAmustikaarumÎncă nu există evaluări
- Reliability and Accuracy of Real-Time Visualization Techniques For Measuring School Cafeteria Tray Waste: Validating The Quarter-Waste MethodDocument5 paginiReliability and Accuracy of Real-Time Visualization Techniques For Measuring School Cafeteria Tray Waste: Validating The Quarter-Waste MethodmustikaarumÎncă nu există evaluări
- Posterior Sagittal Anorectoplasty in Anorectal MalformationsDocument5 paginiPosterior Sagittal Anorectoplasty in Anorectal MalformationsmustikaarumÎncă nu există evaluări
- Ioi 160069Document9 paginiIoi 160069mustikaarumÎncă nu există evaluări
- Hungx BuiDocument92 paginiHungx BuimustikaarumÎncă nu există evaluări
- Nousea and Vomiting Mediciation 130509Document3 paginiNousea and Vomiting Mediciation 130509mustikaarumÎncă nu există evaluări
- Micronutrient and Sam - Am J Clin Nutr-2011-Lemaire-585-93Document9 paginiMicronutrient and Sam - Am J Clin Nutr-2011-Lemaire-585-93mustikaarumÎncă nu există evaluări
- 18 Total Quality ApstractDocument5 pagini18 Total Quality ApstractPooja GuptaÎncă nu există evaluări
- Mustika Arum - 115070300111038 - Application of Hurdles For Extending The Shelf Life of Fresh FruitsDocument18 paginiMustika Arum - 115070300111038 - Application of Hurdles For Extending The Shelf Life of Fresh FruitsmustikaarumÎncă nu există evaluări
- Metronidazole: Common Drug Name Common Brand NamesDocument1 paginăMetronidazole: Common Drug Name Common Brand NamesmustikaarumÎncă nu există evaluări
- Consumer Medicine Information Arrow - Ranitidine: What Is in This LeafletDocument8 paginiConsumer Medicine Information Arrow - Ranitidine: What Is in This LeafletmustikaarumÎncă nu există evaluări
- CircumcisionDocument2 paginiCircumcisionAlvin L. RozierÎncă nu există evaluări
- Lecture 5 Prenatal Genetic CounselingDocument53 paginiLecture 5 Prenatal Genetic Counselingjaish8904Încă nu există evaluări
- Brain Tumors Anatomy Pathology and ManagementDocument16 paginiBrain Tumors Anatomy Pathology and ManagementVanishaÎncă nu există evaluări
- Barbados Credit Unions CoopMED Medical Health InsuranceDocument4 paginiBarbados Credit Unions CoopMED Medical Health InsuranceKammieÎncă nu există evaluări
- HBOC Family History Collection ToolDocument4 paginiHBOC Family History Collection ToolNational Coalition for Health Professional Education in GeneticsÎncă nu există evaluări
- Intracranial TumoursDocument17 paginiIntracranial TumoursYarra Sri HarikaÎncă nu există evaluări
- Chapter 5: Chemicals For Consumers Answer A: Soap and Detergent Activity 1Document6 paginiChapter 5: Chemicals For Consumers Answer A: Soap and Detergent Activity 1Wei FungÎncă nu există evaluări
- Pilonodular Synovitis 2Document19 paginiPilonodular Synovitis 2Madhan Mohan Reddy KatikareddyÎncă nu există evaluări
- Imaging Presacral MassesDocument102 paginiImaging Presacral Masseskiran_mmc100% (2)
- Hipertensi PulmonalDocument15 paginiHipertensi Pulmonaldevi efrinaÎncă nu există evaluări
- Role of Teacher in School Health Education: by Rasheeda, Sabana, Raifa, NethraDocument15 paginiRole of Teacher in School Health Education: by Rasheeda, Sabana, Raifa, NethraJaved Abdul JaleelÎncă nu există evaluări
- Patient Specific Dental Hygiene Care PlanDocument8 paginiPatient Specific Dental Hygiene Care Planapi-354959885Încă nu există evaluări
- The Use of A Reverse Flow Sural Fasciocutaneous Flap in A Patient With Multiple Trauma: A CaseDocument5 paginiThe Use of A Reverse Flow Sural Fasciocutaneous Flap in A Patient With Multiple Trauma: A CasewennyÎncă nu există evaluări
- Cervicothoracic Sign - Print Friendly - STATdxDocument3 paginiCervicothoracic Sign - Print Friendly - STATdxmihaelaÎncă nu există evaluări
- Adenocarcinoma PulmonarDocument75 paginiAdenocarcinoma PulmonarLigia Micaela García XitamulÎncă nu există evaluări
- Bowel Preparation Colon ResectionDocument28 paginiBowel Preparation Colon ResectioncristiangallardovÎncă nu există evaluări
- Phytochemical Information and Pharmacological Activities Of-OkraDocument9 paginiPhytochemical Information and Pharmacological Activities Of-OkraVanThanh DoÎncă nu există evaluări
- B6 Review Exam QuestionsDocument14 paginiB6 Review Exam QuestionsParam BhimaniÎncă nu există evaluări
- Gallbladder Case StudyDocument19 paginiGallbladder Case StudyIan CiarÎncă nu există evaluări