S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- In Vitro Chromosomal AberrationsDocument15 paginiIn Vitro Chromosomal AberrationsdrlandgeÎncă nu există evaluări
- Congenital and Genetic DiseasesDocument84 paginiCongenital and Genetic Diseasesdrlandge100% (1)
- Chromosomal DisordersDocument40 paginiChromosomal Disordersrudette726100% (1)
- Recent Developments in Cytogenetics. (22-10-2001)Document2 paginiRecent Developments in Cytogenetics. (22-10-2001)Dr.Mrs.Krishnaja A. P.Încă nu există evaluări
- Alteration in Number: Autosomal DisordersDocument6 paginiAlteration in Number: Autosomal DisordersnkivcÎncă nu există evaluări
- Bio Mechanics of GAITDocument10 paginiBio Mechanics of GAITRuth RukhsanaÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Chapter 56 Conservation Biology and Restoration EcologyDocument4 paginiChapter 56 Conservation Biology and Restoration EcologyAndyÎncă nu există evaluări
- As Paper2 总msDocument313 paginiAs Paper2 总ms唐雅慧Încă nu există evaluări
- Molecules: The New Challenge of Green Cosmetics: Natural Food Ingredients For Cosmetic FormulationsDocument28 paginiMolecules: The New Challenge of Green Cosmetics: Natural Food Ingredients For Cosmetic FormulationsalbertoÎncă nu există evaluări
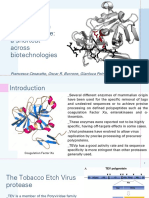
- Tobacco Etch Virus Protease: A Shortcut Across BiotechnologiesDocument16 paginiTobacco Etch Virus Protease: A Shortcut Across BiotechnologiesNhật ThiệnÎncă nu există evaluări
- Rajayakshma: DR B K SevatkarDocument31 paginiRajayakshma: DR B K SevatkarBalkrishan SevatkarÎncă nu există evaluări
- Fetal Developmental MilestonesDocument28 paginiFetal Developmental MilestonesShahad HakimuddinÎncă nu există evaluări
- IB Biology SL - 2024 Prediction Exam - May 2024 Paper 1Document16 paginiIB Biology SL - 2024 Prediction Exam - May 2024 Paper 1Christy HuynhÎncă nu există evaluări
- Chapter 33: Protein SynthesisDocument64 paginiChapter 33: Protein SynthesisDayledaniel SorvetoÎncă nu există evaluări
- FCPS II CardiologyDocument32 paginiFCPS II CardiologyAamir HamaadÎncă nu există evaluări
- Flowchart GaDocument1 paginăFlowchart GaSidney Bruce ShikiÎncă nu există evaluări
- UPDATED Annotated Cell DiagramDocument3 paginiUPDATED Annotated Cell DiagramJ pÎncă nu există evaluări
- Short Notes Form 4 Biology (Chapter 1-4)Document6 paginiShort Notes Form 4 Biology (Chapter 1-4)Ema Fatimah75% (8)
- WAEC BIOLOGY SyllabusDocument78 paginiWAEC BIOLOGY SyllabusMaggieÎncă nu există evaluări
- Theoretical Evolutionary Genetics. Joseph Felsenstein (2016)Document533 paginiTheoretical Evolutionary Genetics. Joseph Felsenstein (2016)Raúl Martín100% (1)
- Awaiting A New DarwinDocument10 paginiAwaiting A New DarwinzizekÎncă nu există evaluări
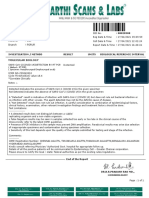
- Gopu.R:::: Patient Age / Sex 30 Y / Male BranchDocument1 paginăGopu.R:::: Patient Age / Sex 30 Y / Male BranchGopu RÎncă nu există evaluări
- Plant ReproductionDocument21 paginiPlant ReproductiondhonaÎncă nu există evaluări
- AP Biology Lab Eight: Population GeneticsDocument9 paginiAP Biology Lab Eight: Population GeneticsCoolAsianDude79% (24)
- Lab 6Document19 paginiLab 6nur athilahÎncă nu există evaluări
- TOEFL ReadingDocument7 paginiTOEFL ReadingMaria OrlovaÎncă nu există evaluări
- Fertilization and MaturationDocument21 paginiFertilization and MaturationRenz L. SalumbreÎncă nu există evaluări
- Biology Chapter 1 Notes (Grade 11)Document4 paginiBiology Chapter 1 Notes (Grade 11)Tammy Lam100% (11)
- Viral Genetics PDFDocument37 paginiViral Genetics PDFTemu Pisah100% (1)
- Submitted in Partial Fulfillment of The Requirement For The Award of The Degree ofDocument47 paginiSubmitted in Partial Fulfillment of The Requirement For The Award of The Degree ofGaurav KÎncă nu există evaluări
- Studentdatainterp Sexual-SelectionDocument5 paginiStudentdatainterp Sexual-SelectionParnoor SinghÎncă nu există evaluări
- PCR LectureDocument35 paginiPCR LectureArfan Tri KusumaÎncă nu există evaluări
- Bugs & DrugsDocument33 paginiBugs & Drugsveronica100% (1)
- Genetic AlgorithmDocument6 paginiGenetic AlgorithmFilip MajstorovićÎncă nu există evaluări
- TestBank ch01Document25 paginiTestBank ch01Edison BajramajÎncă nu există evaluări