S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Presentation5 EV ArchitectureDocument26 paginiPresentation5 EV ArchitectureJAYKUMAR MUKESHBHAI THAKORÎncă nu există evaluări
- 23AE23 DS enDocument4 pagini23AE23 DS enBhageerathi SahuÎncă nu există evaluări
- OVA37066E: Product Data SheetDocument2 paginiOVA37066E: Product Data SheetFred BionÎncă nu există evaluări
- Computational Neuroscience CW1 (Bristol)Document3 paginiComputational Neuroscience CW1 (Bristol)libannfÎncă nu există evaluări
- Cat Hammers C842898Document8 paginiCat Hammers C842898maggioraÎncă nu există evaluări
- Ap Unit 1 NotesDocument42 paginiAp Unit 1 NotesDhruv GoyalÎncă nu există evaluări
- Refining Corrosion Technologist NACE-RCT-001: NACE Cathodic Protection Technician (CP 2) Written ExamDocument16 paginiRefining Corrosion Technologist NACE-RCT-001: NACE Cathodic Protection Technician (CP 2) Written Examshoaib1985100% (1)
- Triosonate in F (TWV 42-F7)Document17 paginiTriosonate in F (TWV 42-F7)EDMILSON BRUNO DO NASCIMENTOÎncă nu există evaluări
- 10048-PAVE-RPT-0101 Types of The Vehicle Considered, Vehicle Details and Single Equivalent Load and Reprtions of LoadDocument14 pagini10048-PAVE-RPT-0101 Types of The Vehicle Considered, Vehicle Details and Single Equivalent Load and Reprtions of LoaddarshanÎncă nu există evaluări
- Kids Curriculum BreakdownDocument6 paginiKids Curriculum BreakdownSuniel ChhetriÎncă nu există evaluări
- Virgil Ionescu Eforie 2016Document99 paginiVirgil Ionescu Eforie 2016Andreea CimpoiÎncă nu există evaluări
- Review Paper - Evolution of CMOS Ring OscillatorDocument10 paginiReview Paper - Evolution of CMOS Ring OscillatorNor Samida YaacobÎncă nu există evaluări
- 3 Perform Industry CalculationsDocument90 pagini3 Perform Industry CalculationsRobinson ConcordiaÎncă nu există evaluări
- Introducing Small Basic-1 PDFDocument69 paginiIntroducing Small Basic-1 PDFnilaÎncă nu există evaluări
- A334 Carino, Patricia Andrea Assignment On ForecastingDocument3 paginiA334 Carino, Patricia Andrea Assignment On ForecastingPatricia Andrea CariñoÎncă nu există evaluări
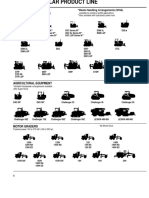
- Caterpillar Product Line 13Document7 paginiCaterpillar Product Line 13GenneraalÎncă nu există evaluări
- HPC168 Passenger CounterDocument9 paginiHPC168 Passenger CounterRommel GómezÎncă nu există evaluări
- Astm - D573.25993Document6 paginiAstm - D573.25993Bryan de BarrosÎncă nu există evaluări
- RCC-DI-AC PipeDocument10 paginiRCC-DI-AC PipeNaveen NagisettiÎncă nu există evaluări
- Sti260N6F6 Stp260N6F6: N-Channel 60 V, 0.0024 Ω, 120 A Stripfet™ Vi Deepgate™ Power Mosfet In To-220 And I²Pak PackagesDocument14 paginiSti260N6F6 Stp260N6F6: N-Channel 60 V, 0.0024 Ω, 120 A Stripfet™ Vi Deepgate™ Power Mosfet In To-220 And I²Pak PackagesRyn YahuFÎncă nu există evaluări
- Gauss Method - Nisan 15Document1 paginăGauss Method - Nisan 15Otis ArmsÎncă nu există evaluări
- Bodybuilder Guidelines: Update: 2011-22Document438 paginiBodybuilder Guidelines: Update: 2011-22thkimzone73100% (12)
- CATIA COMPOSER SYNC2 FLYER 2014 Draft2Document2 paginiCATIA COMPOSER SYNC2 FLYER 2014 Draft2타키비Încă nu există evaluări
- 2010 Jan-01Document32 pagini2010 Jan-01Shine PrabhakaranÎncă nu există evaluări
- Graphite PropertiesDocument42 paginiGraphite PropertiesAnnisa Puspa MustikaÎncă nu există evaluări
- 8 Coil PWM Drivers PDFDocument4 pagini8 Coil PWM Drivers PDFDuzng Hoang TriÎncă nu există evaluări
- Integrals - Integral Calculus - Math - Khan Academy PDFDocument7 paginiIntegrals - Integral Calculus - Math - Khan Academy PDFroberteleeroyÎncă nu există evaluări
- Ugc Model Curriculum Statistics: Submitted To The University Grants Commission in April 2001Document101 paginiUgc Model Curriculum Statistics: Submitted To The University Grants Commission in April 2001Alok ThakkarÎncă nu există evaluări
- Data Download CMM366A-4G V1.0 enDocument16 paginiData Download CMM366A-4G V1.0 enSuramanÎncă nu există evaluări