S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Ghanie Irwan 2019 J. Phys.: Conf. Ser. 1246 012019Document9 paginiGhanie Irwan 2019 J. Phys.: Conf. Ser. 1246 012019mellysa iskandarÎncă nu există evaluări
- GHSB2024 Superficial Structures of The Neck and Posterior TriangleDocument5 paginiGHSB2024 Superficial Structures of The Neck and Posterior Trianglekang seulgi can set me on fire with her gaze aloneÎncă nu există evaluări
- Therefore "Weakness" DOES NOT Help To Establish Whether It Is UMN or LMN lesion-FOLLOWING Pattern of Signs Help Us To EstablishDocument66 paginiTherefore "Weakness" DOES NOT Help To Establish Whether It Is UMN or LMN lesion-FOLLOWING Pattern of Signs Help Us To EstablishBaishakhi ChakrabortyÎncă nu există evaluări
- Wells Partial Denture ProsthodonticsDocument10 paginiWells Partial Denture Prosthodonticsthesabarmo100% (1)
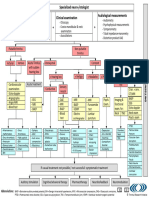
- TRI Tinnitus FlowchartDocument1 paginăTRI Tinnitus FlowchartAdvocacia VitóriaÎncă nu există evaluări
- RespiratoryanatomyDocument5 paginiRespiratoryanatomyMary♡Încă nu există evaluări
- INTERNS NOTES - OtorhinolaryngologyDocument15 paginiINTERNS NOTES - OtorhinolaryngologyKarl Jimenez SeparaÎncă nu există evaluări
- Direct Gingivoperiosteoplasty With PalatoplastyDocument6 paginiDirect Gingivoperiosteoplasty With PalatoplastyAndrés Faúndez TeránÎncă nu există evaluări
- Cleft Lip DR RituDocument82 paginiCleft Lip DR RituRitu SamdyanÎncă nu există evaluări
- Clinical Skills Cranial Nerves I To VI Students Copy 2019Document4 paginiClinical Skills Cranial Nerves I To VI Students Copy 2019carlosÎncă nu există evaluări
- Chapter 11 Sense OrgansDocument18 paginiChapter 11 Sense OrgansMichael Oconnor100% (2)
- Lec 1 Functional Areas of Cerebral CortexDocument37 paginiLec 1 Functional Areas of Cerebral CortexMudassar RoomiÎncă nu există evaluări
- The Function of TongueDocument11 paginiThe Function of TongueAndrea LawÎncă nu există evaluări
- Unit 1 PDF People PDFDocument12 paginiUnit 1 PDF People PDFCosmic LatteÎncă nu există evaluări
- HearingDocument15 paginiHearingdisha mangeÎncă nu există evaluări
- 008 164 Anatomy of Thyroid Gland PDFDocument10 pagini008 164 Anatomy of Thyroid Gland PDFWILLIAMÎncă nu există evaluări
- The Role of Intratympanic Dexamethasone in Sudden Sensorineural Hearing LossDocument5 paginiThe Role of Intratympanic Dexamethasone in Sudden Sensorineural Hearing LossAditya HendraÎncă nu există evaluări
- Salivary GlandsDocument97 paginiSalivary GlandsSwati George100% (2)
- Chapter 8-SPECIAL SENSESDocument5 paginiChapter 8-SPECIAL SENSESrishellemaepilonesÎncă nu există evaluări
- Weinberg2001 THERAPEUTIC BIOMECHANICS CONCEPTS AND CLINICAL PROCEDURES TO REDUCE IMPLANT LOADING. PART II - THERAPEUTIC DIFFERENTIAL LOADINGDocument9 paginiWeinberg2001 THERAPEUTIC BIOMECHANICS CONCEPTS AND CLINICAL PROCEDURES TO REDUCE IMPLANT LOADING. PART II - THERAPEUTIC DIFFERENTIAL LOADINGPablo Gutiérrez Da VeneziaÎncă nu există evaluări
- PonsDocument61 paginiPonsAyberk ZorluÎncă nu există evaluări
- Occlusion in FPDDocument38 paginiOcclusion in FPDDRPRIYA007100% (4)
- Anatomy of The EarDocument10 paginiAnatomy of The EarJP SouaidÎncă nu există evaluări
- TAOMS20 Abstract BookDocument238 paginiTAOMS20 Abstract BookTaha ÖzerÎncă nu există evaluări
- Anatomy Topography of The EyeDocument46 paginiAnatomy Topography of The Eyeikayapmd100% (1)
- HANDOUT Laryngeal-MassageDocument7 paginiHANDOUT Laryngeal-MassageAnca OÎncă nu există evaluări
- MRI & CT of Facial Bones PDFDocument53 paginiMRI & CT of Facial Bones PDFdr_340802071Încă nu există evaluări
- Assessing The Nose and Sinuses: Return Demonstration Tool Evaluation ForDocument3 paginiAssessing The Nose and Sinuses: Return Demonstration Tool Evaluation Forclint xavier odangoÎncă nu există evaluări
- Patient Type: OPD: TSH Test ReportDocument1 paginăPatient Type: OPD: TSH Test ReportVeenu SehrawatÎncă nu există evaluări
- Kadasne's Textbook of Anatomy (Clinically Oriented) VOLUME 3 Head, Neck, Face and Brain (2009) (PDF) (UnitedVRG)Document365 paginiKadasne's Textbook of Anatomy (Clinically Oriented) VOLUME 3 Head, Neck, Face and Brain (2009) (PDF) (UnitedVRG)Ahmad YÎncă nu există evaluări