S-ar putea să vă placă și
- Chapter 5 in The Beginning - The Cosmic EggDocument4 paginiChapter 5 in The Beginning - The Cosmic EggMaria TountaÎncă nu există evaluări
- 9 FCFD 50 Ad 768 e 57178Document75 pagini9 FCFD 50 Ad 768 e 57178Maria TountaÎncă nu există evaluări
- GBB 12109Document18 paginiGBB 12109Maria TountaÎncă nu există evaluări
- History of BrainDocument3 paginiHistory of BrainMaria TountaÎncă nu există evaluări
- 29Document1 pagină29Maria TountaÎncă nu există evaluări
- Vocabulary of EmotionsDocument1 paginăVocabulary of EmotionsDouble_G100% (50)
- GBB 12109Document18 paginiGBB 12109Maria TountaÎncă nu există evaluări
- I Ching Hex 34Document3 paginiI Ching Hex 34Maria TountaÎncă nu există evaluări
- Clean Space - Modeling Human Perception Through Emergence by Penny Tompkins & James LawleyDocument9 paginiClean Space - Modeling Human Perception Through Emergence by Penny Tompkins & James LawleyMaria TountaÎncă nu există evaluări
- Kurtz - Development of Hakomi PDFDocument11 paginiKurtz - Development of Hakomi PDFmax00ha100% (1)
- I Ching - Hex 18Document4 paginiI Ching - Hex 18Maria TountaÎncă nu există evaluări
- A Basic Buddhism Guide - Dependent ArisingDocument7 paginiA Basic Buddhism Guide - Dependent ArisingMaria TountaÎncă nu există evaluări
- Perry Handout Effects of TraumaDocument21 paginiPerry Handout Effects of TraumaMaria Tounta100% (3)
- MeaningBehavioural EconomicsDocument7 paginiMeaningBehavioural EconomicstukifÎncă nu există evaluări
- Buddhism and EmpiricismDocument5 paginiBuddhism and EmpiricismMaria TountaÎncă nu există evaluări
- Erik Erikson, 91, Psychoanalyst Who Reshaped Views of Human Growth, Dies - New York TimesDocument5 paginiErik Erikson, 91, Psychoanalyst Who Reshaped Views of Human Growth, Dies - New York TimesMaria TountaÎncă nu există evaluări
- Bartlett, ExperimentsDocument19 paginiBartlett, ExperimentsMaria TountaÎncă nu există evaluări
- MacLeod 1991Document41 paginiMacLeod 1991Maria TountaÎncă nu există evaluări
- WaterDocument1 paginăWaterMaria TountaÎncă nu există evaluări
- WaterDocument1 paginăWaterMaria TountaÎncă nu există evaluări
- Erik Erikson, 91, Psychoanalyst Who Reshaped Views of Human Growth, Dies - New York TimesDocument5 paginiErik Erikson, 91, Psychoanalyst Who Reshaped Views of Human Growth, Dies - New York TimesMaria TountaÎncă nu există evaluări
- Odes SeyDocument6 paginiOdes SeyMaria TountaÎncă nu există evaluări
- FreudDocument15 paginiFreudMaria TountaÎncă nu există evaluări
- Buddhism and EmpiricismDocument5 paginiBuddhism and EmpiricismMaria TountaÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Neurotransmitters PDFDocument23 paginiNeurotransmitters PDFБакытÎncă nu există evaluări
- Basal Ganglia (Edit)Document66 paginiBasal Ganglia (Edit)kkkaadashfisafÎncă nu există evaluări
- Lecture 30 Histology of CnsDocument56 paginiLecture 30 Histology of CnsJustin DawsonÎncă nu există evaluări
- Understanding Ulnar Nerve Injuries and AnatomyDocument18 paginiUnderstanding Ulnar Nerve Injuries and Anatomynihal adriel gomesÎncă nu există evaluări
- Clinical Skills Cranial Nerves I To VI Students Copy 2019Document4 paginiClinical Skills Cranial Nerves I To VI Students Copy 2019carlosÎncă nu există evaluări
- Clinical Approach To Brainstem LesionsDocument10 paginiClinical Approach To Brainstem LesionsJosé SánchezÎncă nu există evaluări
- Charcot-Marie-Tooth DiseaseDocument2 paginiCharcot-Marie-Tooth DiseaseitsmeayaeÎncă nu există evaluări
- Referred PainDocument18 paginiReferred Painapi-3710331Încă nu există evaluări
- ACT Personal Trainer Certification Textbook v1 2Document315 paginiACT Personal Trainer Certification Textbook v1 2AwyrMerddyn100% (7)
- MPhil Thesis Tharaka DassanayakeDocument185 paginiMPhil Thesis Tharaka DassanayakeAnand RasaneÎncă nu există evaluări
- Reflex ArcDocument8 paginiReflex ArcHina AsifÎncă nu există evaluări
- Primitive Streak Notochord FormationDocument41 paginiPrimitive Streak Notochord FormationCsongiÎncă nu există evaluări
- Nervous SystemDocument23 paginiNervous SystemBryan Bries100% (1)
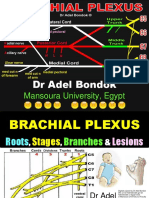
- Brachial Plexus, DR Adel BondokDocument20 paginiBrachial Plexus, DR Adel BondokSafeÎncă nu există evaluări
- 2402 Lab - Reflex PhysiolDocument4 pagini2402 Lab - Reflex PhysiolClarisse AnneÎncă nu există evaluări
- Neural Transmission: Chapter ThreeDocument1 paginăNeural Transmission: Chapter ThreeBoitor ValerianÎncă nu există evaluări
- DR Bhatia Medical Coaching Institute: NeuroanatomyDocument3 paginiDR Bhatia Medical Coaching Institute: NeuroanatomyAastha JainÎncă nu există evaluări
- Anatomy MnemonicsDocument3 paginiAnatomy MnemonicsAbc AbcÎncă nu există evaluări
- The Posterior Fossa Cisterns: Albert L. Rhoton, JR., M.DDocument12 paginiThe Posterior Fossa Cisterns: Albert L. Rhoton, JR., M.DIndra HadianditeÎncă nu există evaluări
- Clinical Aspects of UMN LMNDocument24 paginiClinical Aspects of UMN LMNKelly YeowÎncă nu există evaluări
- Neurology II 2.07 Pain Dr. Camara ChuaDocument24 paginiNeurology II 2.07 Pain Dr. Camara ChuaDanica Nicole Seco GabonÎncă nu există evaluări
- Chiari MalformationDocument3 paginiChiari MalformationAloysius RodriguesÎncă nu există evaluări
- Sem-3 Physiology of PainDocument69 paginiSem-3 Physiology of PainJyoti Pol SherkhaneÎncă nu există evaluări
- Cerebellum Essay - Connections and Functions of The CerebellumDocument4 paginiCerebellum Essay - Connections and Functions of The CerebellumscholifyÎncă nu există evaluări
- The Cisterna Magna SeptaDocument13 paginiThe Cisterna Magna SeptaFrancisco A. Villegas-LópezÎncă nu există evaluări
- Cranial NervesDocument16 paginiCranial Nervesapi-302547403100% (1)
- Bells PalsyDocument6 paginiBells PalsyElisabeth TikalakaÎncă nu există evaluări
- Cephalopod Neural NetworksDocument12 paginiCephalopod Neural NetworksSabrina Indri WardaniÎncă nu există evaluări
- Brainstem Rule of 4Document11 paginiBrainstem Rule of 4Anonymous 0gUash0BxÎncă nu există evaluări
- Brain, Parts and FunctionsDocument2 paginiBrain, Parts and FunctionsMiss AÎncă nu există evaluări