S-ar putea să vă placă și
- Authorization To Treat Mechanical Ventilator: Resuscitation and The Proper Use of A Manual Resuscitation DeviceDocument1 paginăAuthorization To Treat Mechanical Ventilator: Resuscitation and The Proper Use of A Manual Resuscitation DeviceAccreditation ConsultantÎncă nu există evaluări
- 1003 - Informed ConsentDocument5 pagini1003 - Informed ConsentAccreditation ConsultantÎncă nu există evaluări
- 08 - Privileges - PaDocument2 pagini08 - Privileges - PaAccreditation ConsultantÎncă nu există evaluări
- 08 - Privileges - Orthopaedics SurgeryDocument3 pagini08 - Privileges - Orthopaedics SurgeryAccreditation ConsultantÎncă nu există evaluări
- 1000-Ca Retail License and ExempteesDocument1 pagină1000-Ca Retail License and ExempteesAccreditation ConsultantÎncă nu există evaluări
- 08 - Privileges - General SurgeryDocument3 pagini08 - Privileges - General SurgeryAccreditation ConsultantÎncă nu există evaluări
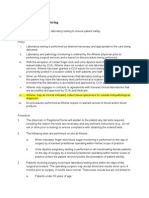
- 3 7 Laboratory MonitoringDocument2 pagini3 7 Laboratory MonitoringAccreditation ConsultantÎncă nu există evaluări
- Laser Plan & Policy 2011Document14 paginiLaser Plan & Policy 2011Accreditation ConsultantÎncă nu există evaluări
- 1 Senior Home Health Employee HandbookDocument77 pagini1 Senior Home Health Employee HandbookAccreditation ConsultantÎncă nu există evaluări
- Rights: THE of Our Patients, and TheirDocument3 paginiRights: THE of Our Patients, and TheirAccreditation ConsultantÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Gastrointestinal Stress Ulcer Prophylaxis GuidelinesDocument4 paginiGastrointestinal Stress Ulcer Prophylaxis GuidelinesAty DwijayantiÎncă nu există evaluări
- SwotDocument3 paginiSwotKimberley Anne SantosÎncă nu există evaluări
- Final AnalysisDocument2 paginiFinal Analysisapi-478583234Încă nu există evaluări
- Organization of A Neonatal Intensive Care UnitDocument30 paginiOrganization of A Neonatal Intensive Care UnitJaya Prabha90% (29)
- Levine Nursing Theory PresentationDocument39 paginiLevine Nursing Theory PresentationMadzni LoquiasÎncă nu există evaluări
- Wa0011.Document10 paginiWa0011.SojiÎncă nu există evaluări
- Draping of Tibia: With An Extremity DrapeDocument2 paginiDraping of Tibia: With An Extremity Drapebagus lazuardiÎncă nu există evaluări
- Journal Thesis 1Document8 paginiJournal Thesis 1bambangÎncă nu există evaluări
- About Our Children, July 2014Document21 paginiAbout Our Children, July 2014New Jersey Jewish StandardÎncă nu există evaluări
- Fresh Call Up Instrs TES 43Document16 paginiFresh Call Up Instrs TES 43Ananta Saran NayakÎncă nu există evaluări
- MP 13212Document15 paginiMP 13212Mauro Rojas ZúñigaÎncă nu există evaluări
- KONSELING DOSEN Beginning A RelationshipDocument30 paginiKONSELING DOSEN Beginning A RelationshipfaiqÎncă nu există evaluări
- Burnout Research 2019 AbellabnosaDocument16 paginiBurnout Research 2019 AbellabnosaRex Decolongon Jr.100% (1)
- SOP1 - Hospital Security and Safety ManagementDocument6 paginiSOP1 - Hospital Security and Safety ManagementParind Phaldesai100% (7)
- Modern Slavery GNRCDocument6 paginiModern Slavery GNRCRitesh SidamÎncă nu există evaluări
- Notes On Nursing (Nightingale, Florence) (Z-Library) PDFDocument195 paginiNotes On Nursing (Nightingale, Florence) (Z-Library) PDFanaÎncă nu există evaluări
- Grp. 4 - BGCDocument15 paginiGrp. 4 - BGCVanessa TyÎncă nu există evaluări
- Steps of The A3 ProcessDocument14 paginiSteps of The A3 ProcessJayantRKÎncă nu există evaluări
- Medi Assist Claim FormDocument6 paginiMedi Assist Claim Formharezzebra0% (2)
- Nusing Skills Output (Nso)Document3 paginiNusing Skills Output (Nso)leroux2890Încă nu există evaluări
- Lovelace Bed-Sharing LetterDocument2 paginiLovelace Bed-Sharing Lettertdingmann3869Încă nu există evaluări
- Burn UnitDocument206 paginiBurn UnitJeisson Osorio Trujillo100% (1)
- Patton FullerDocument5 paginiPatton FullerJacques OwokelÎncă nu există evaluări
- Consultation-Liaison Psychiatry (Psychosomatic Medicine) : M.Zainie Hassan A.RDocument25 paginiConsultation-Liaison Psychiatry (Psychosomatic Medicine) : M.Zainie Hassan A.RDavi DzikirianÎncă nu există evaluări
- Real World Endo Sequence FileDocument24 paginiReal World Endo Sequence FileFernando CordovaÎncă nu există evaluări
- Planning and Organizing of HospitalDocument36 paginiPlanning and Organizing of HospitalMamta Poonia100% (1)
- BeneFusion VP5 FP Operator's Manual V2.0 enDocument114 paginiBeneFusion VP5 FP Operator's Manual V2.0 enherbertamaya0% (1)
- Innovation in Nursing PracticesDocument6 paginiInnovation in Nursing PracticesVijaya RaniÎncă nu există evaluări
- Csi Cardiology Update 2018 Binder 1Document1.160 paginiCsi Cardiology Update 2018 Binder 1nikhil100% (1)
- FY2009 State Grants AllDocument1.117 paginiFY2009 State Grants AllPrattvilleRevolutionÎncă nu există evaluări