S-ar putea să vă placă și
- Cardiovascular System - 4th EdDocument201 paginiCardiovascular System - 4th EdDjennyDerane100% (3)
- UP PGH 2019 Interns Review 1 Benign GyneDocument152 paginiUP PGH 2019 Interns Review 1 Benign GyneTrisÎncă nu există evaluări
- Embryology of The HeartDocument16 paginiEmbryology of The HeartRut H. P. EkasiwiÎncă nu există evaluări
- Cardiovascular Clinical ExaminationDocument27 paginiCardiovascular Clinical ExaminationAshiniÎncă nu există evaluări
- EKG IntroductionDocument28 paginiEKG IntroductionJj JungÎncă nu există evaluări
- ... 4 Finals Cardiovascular PhysiologyDocument8 pagini... 4 Finals Cardiovascular PhysiologyELIZABETH GRACE AMADORÎncă nu există evaluări
- Platinum Notes - Anatomy (2014-15)Document88 paginiPlatinum Notes - Anatomy (2014-15)Priyanka ShanmugamÎncă nu există evaluări
- AHA The ECG Examination PDFDocument41 paginiAHA The ECG Examination PDFSaeful AnwarudinÎncă nu există evaluări
- Embryology of The Heart and The Great VesselsDocument66 paginiEmbryology of The Heart and The Great VesselsNavya HegdeÎncă nu există evaluări
- Chapter 26 Management of Patients With Dysrhythmias and Conduction ProblemsDocument22 paginiChapter 26 Management of Patients With Dysrhythmias and Conduction ProblemsAbel C. Idusma Jr.Încă nu există evaluări
- Anatomy Comprehensive Exam Review QuestionsDocument22 paginiAnatomy Comprehensive Exam Review QuestionsKlean Jee Teo-TrazoÎncă nu există evaluări
- Cardiology Notes PDFDocument62 paginiCardiology Notes PDFNikos SyrigosÎncă nu există evaluări
- Cardiac Surgical Operative AtlasDe la EverandCardiac Surgical Operative AtlasThorsten WahlersÎncă nu există evaluări
- Anatomy: Heart and PericardiumDocument95 paginiAnatomy: Heart and PericardiumDitas Chu100% (1)
- Robbins - 12 The HeartDocument5 paginiRobbins - 12 The HeartCM NajitoÎncă nu există evaluări
- Cronic Heart Failure - EscDocument55 paginiCronic Heart Failure - EscRisti Graharti100% (1)
- Electrocardiogram (E.C.G)Document51 paginiElectrocardiogram (E.C.G)Jamuna PatelÎncă nu există evaluări
- STEMI Equivalents: DR Elesia Powell-Williams Emergency Medicine Resident PGY3Document39 paginiSTEMI Equivalents: DR Elesia Powell-Williams Emergency Medicine Resident PGY3elesia powell100% (1)
- Kidney Kard - 6th EditionDocument4 paginiKidney Kard - 6th EditionHamlot100% (1)
- One Shot ANATOMY Revision by DR Ashwani KumarDocument94 paginiOne Shot ANATOMY Revision by DR Ashwani KumarTauqueer AlamÎncă nu există evaluări
- Pakya ECG BasicsDocument5 paginiPakya ECG BasicsFrederick CokroÎncă nu există evaluări
- Cardio Day 1 TemplateDocument18 paginiCardio Day 1 TemplateMikeÎncă nu există evaluări
- Dev of CVS-2Document33 paginiDev of CVS-2Vanshika GargÎncă nu există evaluări
- 1.anatomi KVDocument40 pagini1.anatomi KVDiiah AyuÎncă nu există evaluări
- Embrilogi Sist. Kardiovaskular 2.2Document87 paginiEmbrilogi Sist. Kardiovaskular 2.2Tara WifaÎncă nu există evaluări
- Ontogeni Cor: Abd. Razak Datu Department of Anatomy Fac. of Medicine UnhasDocument50 paginiOntogeni Cor: Abd. Razak Datu Department of Anatomy Fac. of Medicine UnhasHadi TryadiÎncă nu există evaluări
- CardiologyDocument220 paginiCardiologyGlorivy E. Mora GonzalezÎncă nu există evaluări
- 2014 Primer 08 Study GuidepdfDocument3 pagini2014 Primer 08 Study GuidepdfThomas MeduneckasÎncă nu există evaluări
- 4 EL Husseinys Essentials of Cardiovascular System @eduwaves360Document236 pagini4 EL Husseinys Essentials of Cardiovascular System @eduwaves360ahmed_abu_alrobÎncă nu există evaluări
- Cardiac Embryology - DR Radit PDFDocument37 paginiCardiac Embryology - DR Radit PDFCandice Lavigne100% (1)
- Cardiovascular System-13 (Muhadharaty)Document51 paginiCardiovascular System-13 (Muhadharaty)maysanitmaysanÎncă nu există evaluări
- Cardiovascular SystemDocument5 paginiCardiovascular Systemy30ny30nÎncă nu există evaluări
- MSGD6 PDFDocument18 paginiMSGD6 PDFEric Meynard SanchezÎncă nu există evaluări
- Chapter 120. Septation of Ventricles, Truncus Arteriosus, and Conus Cordis - Review of Medical Embryology Book - LifeMap DiscoveDocument1 paginăChapter 120. Septation of Ventricles, Truncus Arteriosus, and Conus Cordis - Review of Medical Embryology Book - LifeMap DiscoveMatthew GiscombeÎncă nu există evaluări
- Annotated OneShotANAT, DR Ashwani - 230208 - 143653Document90 paginiAnnotated OneShotANAT, DR Ashwani - 230208 - 143653KabbuÎncă nu există evaluări
- Vascular SystemDocument8 paginiVascular SystemCassandra Mae PerochoÎncă nu există evaluări
- Development of The HeartDocument27 paginiDevelopment of The HeartJoy KirumbaÎncă nu există evaluări
- Cardiac Conduction System Power Point PresentationDocument30 paginiCardiac Conduction System Power Point PresentationAaya AdelÎncă nu există evaluări
- Kuliah JantungDocument47 paginiKuliah JantungAlmazida fauzil AishaqeenaÎncă nu există evaluări
- Anatomy One Shot DR AshwiniDocument95 paginiAnatomy One Shot DR Ashwinienthusiast383Încă nu există evaluări
- Ariestya Indah Permata Sari: April 2018Document53 paginiAriestya Indah Permata Sari: April 2018gini marta lestariÎncă nu există evaluări
- FA 2020 - Cardio EmbryoDocument7 paginiFA 2020 - Cardio EmbryoDrbee10Încă nu există evaluări
- Anatomy of The Heart - Dr. Wael Amin - 6 March 2024Document33 paginiAnatomy of The Heart - Dr. Wael Amin - 6 March 2024ciyace7849Încă nu există evaluări
- Circulatory System PearsonsDocument16 paginiCirculatory System Pearsonsblando.shaneÎncă nu există evaluări
- Marrow ErrataDocument268 paginiMarrow ErrataDr.Ebenesar DhasarathanÎncă nu există evaluări
- 1 Pericardium - MbbsDocument34 pagini1 Pericardium - MbbsmwadramannÎncă nu există evaluări
- FA 2019 CardiovascularDocument44 paginiFA 2019 CardiovascularLexÎncă nu există evaluări
- HEART-Dr. Fernandez Fluid: Acts As A Lubricant: ND THDocument2 paginiHEART-Dr. Fernandez Fluid: Acts As A Lubricant: ND THMarianne RuizÎncă nu există evaluări
- The Heart & Mediastinum: A Fixed Learning Module 2009 Compiled by Assoc Prof DR Hamiadji TanuseputroDocument40 paginiThe Heart & Mediastinum: A Fixed Learning Module 2009 Compiled by Assoc Prof DR Hamiadji TanuseputroQiqin DechrifentoÎncă nu există evaluări
- The Head and Neck AnatomyDocument39 paginiThe Head and Neck AnatomySwati LataÎncă nu există evaluări
- Development of Heart & Vasculature - Part 1 - F2023 - DR D CostaDocument25 paginiDevelopment of Heart & Vasculature - Part 1 - F2023 - DR D CostaJose PerezÎncă nu există evaluări
- Chapter 12 StudentsDocument6 paginiChapter 12 StudentsJohn Paul CastilloÎncă nu există evaluări
- Head and Neck DevelopmentDocument27 paginiHead and Neck Developmentdagehi6880Încă nu există evaluări
- 14 - Development of CVS-II (Heart) - DR - GosaiDocument52 pagini14 - Development of CVS-II (Heart) - DR - GosaiDr.B.B.GosaiÎncă nu există evaluări
- 01-Anatomy of KidneyDocument32 pagini01-Anatomy of KidneyMRS DR NIDHI SHARMA VISHWAKARMAÎncă nu există evaluări
- NEURULATION N Derivatives FDocument70 paginiNEURULATION N Derivatives Ffilza farheenÎncă nu există evaluări
- Anatomy of The Heart AssignmentDocument10 paginiAnatomy of The Heart AssignmentKarim AL-TijaniÎncă nu există evaluări
- Circulation Lec 2 Part-2Document21 paginiCirculation Lec 2 Part-2Rudrapalash ChakrabartiÎncă nu există evaluări
- Carotid Artery DiseaseDocument48 paginiCarotid Artery DiseaseAdeleye John AdebolaÎncă nu există evaluări
- Hap - Circulatory System HeartDocument13 paginiHap - Circulatory System HeartKyle LumingkitÎncă nu există evaluări
- Heart Anatomy Exam 3Document4 paginiHeart Anatomy Exam 3Amar AlkhafajiÎncă nu există evaluări
- FghjiuytDocument1 paginăFghjiuytYanÎncă nu există evaluări
- Embryonic Angio and Vasculogenesis: BY Dr. Siwa O.BDocument28 paginiEmbryonic Angio and Vasculogenesis: BY Dr. Siwa O.BBeing BipolarÎncă nu există evaluări
- Introduction To Heart Tube FormationDocument33 paginiIntroduction To Heart Tube FormationAarushi JainÎncă nu există evaluări
- 5a - Osteology of Thorax - Intercostal SpacesDocument68 pagini5a - Osteology of Thorax - Intercostal SpacesINTERNET MONEY HACKÎncă nu există evaluări
- Blood Can Be Very Bad (Perron Ich Acep 2005 Peds Course (1) )Document15 paginiBlood Can Be Very Bad (Perron Ich Acep 2005 Peds Course (1) )Moileon2011Încă nu există evaluări
- 200F-21 The Brain SVDocument20 pagini200F-21 The Brain SVRachel SawhÎncă nu există evaluări
- Aik 70084398 - Embryological Development of Fetal HeartDocument20 paginiAik 70084398 - Embryological Development of Fetal HeartUzma ZafarÎncă nu există evaluări
- CARDIO VASCULAR SYSTEM TransesDocument4 paginiCARDIO VASCULAR SYSTEM TransesBianca Paulyn CastilloÎncă nu există evaluări
- Embedded IitdDocument7 paginiEmbedded IitdRobert HornÎncă nu există evaluări
- Routing Protocol For Ad HocDocument10 paginiRouting Protocol For Ad HocRobert HornÎncă nu există evaluări
- Location Aided Routing ProtocolDocument15 paginiLocation Aided Routing ProtocolRobert HornÎncă nu există evaluări
- Mobility Models For Ad HocDocument10 paginiMobility Models For Ad HocRobert HornÎncă nu există evaluări
- Vehicular Ad Hoc NetworksDocument1 paginăVehicular Ad Hoc NetworksRobert HornÎncă nu există evaluări
- Realistic Vehicular Ad-Hoc NetworksDocument6 paginiRealistic Vehicular Ad-Hoc NetworksRobert HornÎncă nu există evaluări
- Cisco CCNP JCacademyDocument1 paginăCisco CCNP JCacademyRobert HornÎncă nu există evaluări
- Red Hat Training and CertificationDocument4 paginiRed Hat Training and CertificationRobert HornÎncă nu există evaluări
- Embeddded Software CertificationDocument4 paginiEmbeddded Software CertificationRobert HornÎncă nu există evaluări
- CCNP ItenablerDocument2 paginiCCNP ItenablerRobert HornÎncă nu există evaluări
- CCNP SpecificationsDocument2 paginiCCNP SpecificationsRobert HornÎncă nu există evaluări
- GNT Nigeria-Ccna BrochureDocument2 paginiGNT Nigeria-Ccna BrochureRobert HornÎncă nu există evaluări
- Embedded Certification-Salzburg UniversityDocument1 paginăEmbedded Certification-Salzburg UniversityRobert HornÎncă nu există evaluări
- CCNA American InteractiveDocument2 paginiCCNA American InteractiveRobert HornÎncă nu există evaluări
- CCNA American InteractiveDocument2 paginiCCNA American InteractiveRobert HornÎncă nu există evaluări
- CCNP ItenablerDocument2 paginiCCNP ItenablerRobert HornÎncă nu există evaluări
- CCNP SpecificationsDocument2 paginiCCNP SpecificationsRobert HornÎncă nu există evaluări
- EmbedAsia BrochureDocument2 paginiEmbedAsia BrochureRobert HornÎncă nu există evaluări
- Industrial Training BrochureDocument4 paginiIndustrial Training BrochureRobert HornÎncă nu există evaluări
- Cisco CCNP JCacademyDocument1 paginăCisco CCNP JCacademyRobert HornÎncă nu există evaluări
- CCNA Discovery DSDocument2 paginiCCNA Discovery DSkovach84Încă nu există evaluări
- At&S CCNA BrochureDocument1 paginăAt&S CCNA BrochureRobert HornÎncă nu există evaluări
- TCS Brochure - Electronics and Embedded SystemsDocument4 paginiTCS Brochure - Electronics and Embedded SystemsRobert HornÎncă nu există evaluări
- CCNA American InteractiveDocument2 paginiCCNA American InteractiveRobert HornÎncă nu există evaluări
- Heart Diesease Hypertension StrokeDocument36 paginiHeart Diesease Hypertension StrokeRobert HornÎncă nu există evaluări
- Cardiac Diesease, A Psychological ApproachDocument37 paginiCardiac Diesease, A Psychological ApproachRobert HornÎncă nu există evaluări
- Is A Muscle About The Size of Your Fist - WeighsDocument24 paginiIs A Muscle About The Size of Your Fist - WeighsRobert HornÎncă nu există evaluări
- CS1998Document16 paginiCS1998api-3755123Încă nu există evaluări
- Heart The Silent KillerDocument41 paginiHeart The Silent KillerRobert HornÎncă nu există evaluări
- DigoxinDocument4 paginiDigoxinKat ZÎncă nu există evaluări
- Atrial Septal DefectDocument3 paginiAtrial Septal Defectmu_crÎncă nu există evaluări
- Renal Vascular Diseases FinalDocument43 paginiRenal Vascular Diseases FinalAlina CazanÎncă nu există evaluări
- Nursing Functions: Daily Routine Sebastian Villalba NossaDocument23 paginiNursing Functions: Daily Routine Sebastian Villalba NossaSebasCdlmÎncă nu există evaluări
- Eec Prague 2017 Program, European Echocardiography Course On Congenital Heart Disease, October 2017Document7 paginiEec Prague 2017 Program, European Echocardiography Course On Congenital Heart Disease, October 2017Navojit ChowdhuryÎncă nu există evaluări
- Stop-Acei Trial Journal ClubDocument3 paginiStop-Acei Trial Journal Clubapi-648891519Încă nu există evaluări
- Pu Control Normal Lot 525 14601 Ed 2/29/2024Document3 paginiPu Control Normal Lot 525 14601 Ed 2/29/2024Ulfa SanofaÎncă nu există evaluări
- Nature Review, Complete RevascularizationDocument14 paginiNature Review, Complete RevascularizationIván De LeónÎncă nu există evaluări
- Basic Principles of Normal ECG: Prepared By: Ben Ryan Jucay SauceDocument25 paginiBasic Principles of Normal ECG: Prepared By: Ben Ryan Jucay SauceSoySauceÎncă nu există evaluări
- TMSDocument2 paginiTMSrapgabrielÎncă nu există evaluări
- Clinical Indication Def.Document11 paginiClinical Indication Def.Anish H DaveÎncă nu există evaluări
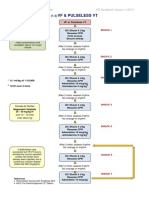
- VF & Pulseless VTDocument1 paginăVF & Pulseless VTmadimadi11Încă nu există evaluări
- ECPD Summer School CVD 2022Document6 paginiECPD Summer School CVD 2022Primalni ZevÎncă nu există evaluări
- Electrical Axis of HeartDocument19 paginiElectrical Axis of Heartrera_avisÎncă nu există evaluări
- Clinical Audit - AcsDocument19 paginiClinical Audit - Acssanisani1020Încă nu există evaluări
- ExaminationofpulseDocument6 paginiExaminationofpulsePeter Paul GollamudiÎncă nu există evaluări
- Total Anomalous Pulmonary Venous Connection (TAPVC)Document2 paginiTotal Anomalous Pulmonary Venous Connection (TAPVC)Tri RachmadijantoÎncă nu există evaluări
- Test Bank For Interpreting Ecgs A Practical Approach 3rd Edition Bruce ShadeDocument11 paginiTest Bank For Interpreting Ecgs A Practical Approach 3rd Edition Bruce ShadeLisaTurnerMDkfym100% (27)
- Hubungan Hipertrigliseridemia Dengan Kadar Kreatinin Pada Pasien Diabetes Melitus Tipe 2 Di RSUD Al-Ihsan Provinsi Jawa Barat Periode Tahun 2014-2015Document8 paginiHubungan Hipertrigliseridemia Dengan Kadar Kreatinin Pada Pasien Diabetes Melitus Tipe 2 Di RSUD Al-Ihsan Provinsi Jawa Barat Periode Tahun 2014-2015Rindani Suci HusnaÎncă nu există evaluări
- The Mechanism Isorhythmic: of Synchronization A-VDocument11 paginiThe Mechanism Isorhythmic: of Synchronization A-VSheila AdiwinataÎncă nu există evaluări
- Jurnal CKDDocument9 paginiJurnal CKDwiwik suprihatinÎncă nu există evaluări