S-ar putea să vă placă și
- Cyanotic Heart DiseaseDocument66 paginiCyanotic Heart DiseasePrasanth SankarÎncă nu există evaluări
- Gerry B. Acosta, MD, FPPS, FPCC: Pediatric CardiologistDocument51 paginiGerry B. Acosta, MD, FPPS, FPCC: Pediatric CardiologistChristian Clyde N. ApigoÎncă nu există evaluări
- Non-Cyanotic Congenital Heart Disease-UpDate 4-22-53Document136 paginiNon-Cyanotic Congenital Heart Disease-UpDate 4-22-53getnusÎncă nu există evaluări
- Approach Cyanosis FinalDocument31 paginiApproach Cyanosis Finalsuheena.CÎncă nu există evaluări
- Eni Rahmawati, S.Kep., NS., M.KepDocument46 paginiEni Rahmawati, S.Kep., NS., M.KepLisa Qoriana RohmaniÎncă nu există evaluări
- Disseminated Intravascular CoagulationDocument16 paginiDisseminated Intravascular CoagulationDocRNÎncă nu există evaluări
- Mnlkaxi QH: Manisha M.Sc. NursingDocument57 paginiMnlkaxi QH: Manisha M.Sc. NursingManisha ShakyaÎncă nu există evaluări
- Gestational Age Related Problems of The Newborn: Carla Reinke, RN, MN, Arnp, CNMDocument120 paginiGestational Age Related Problems of The Newborn: Carla Reinke, RN, MN, Arnp, CNMsulekhaanoobÎncă nu există evaluări
- Fluid Balance and Venous Access in ChildrenDocument51 paginiFluid Balance and Venous Access in Childrenhayssam rashwan100% (1)
- Congenital Anomalies of Ureter BladderDocument17 paginiCongenital Anomalies of Ureter BladderAfiq SabriÎncă nu există evaluări
- Prevention & Treatment of Rop: Presentation: DR Manaswinee Sahoo Guide: DR Swati UpadhyayDocument42 paginiPrevention & Treatment of Rop: Presentation: DR Manaswinee Sahoo Guide: DR Swati Upadhyaypranaya mallÎncă nu există evaluări
- Shock in NeonatesDocument14 paginiShock in NeonatesAbiy AliyeÎncă nu există evaluări
- Cerebral Palsy: and Its Sequelae.. (Consequences)Document143 paginiCerebral Palsy: and Its Sequelae.. (Consequences)Agus SarjonoÎncă nu există evaluări
- Neonatal Seizures: Dr. Venkatesh Postgraduate Dept of Pediatrics S V Medical CollegeDocument43 paginiNeonatal Seizures: Dr. Venkatesh Postgraduate Dept of Pediatrics S V Medical CollegeManju ManjunathÎncă nu există evaluări
- Cerebrospinal Meningitis (CSM) : Adwoa Baffour AwuahDocument38 paginiCerebrospinal Meningitis (CSM) : Adwoa Baffour AwuahMichael Adjei100% (1)
- Skeletal SystemDocument66 paginiSkeletal SystemEDLYN BRAZILÎncă nu există evaluări
- Respiratory System - 2019Document20 paginiRespiratory System - 2019Glen Lazarus100% (1)
- Cystic Diseases of KidneyDocument12 paginiCystic Diseases of Kidneymnr hmcÎncă nu există evaluări
- Congenital Heart DiseasesDocument27 paginiCongenital Heart DiseasesJumar ValdezÎncă nu există evaluări
- Approach To Ill Looking ChildDocument66 paginiApproach To Ill Looking ChildUzair MuhdÎncă nu există evaluări
- 12 Neonatal Hypocalcemia, Glycemia and MagnesemiaDocument55 pagini12 Neonatal Hypocalcemia, Glycemia and MagnesemiaRana Vandana100% (1)
- Eb SteinDocument112 paginiEb SteinAsena TuiketeiÎncă nu există evaluări
- Heart Failure in ChildhoodDocument43 paginiHeart Failure in Childhoodhusnajihah18Încă nu există evaluări
- Cyanosis in The NewbornDocument32 paginiCyanosis in The Newbornimma_2014Încă nu există evaluări
- Congenital Development of Urinary SystemDocument31 paginiCongenital Development of Urinary SystemRinxas VerinxtÎncă nu există evaluări
- Anemia in Newborn BabyDocument10 paginiAnemia in Newborn BabyfroziillahiÎncă nu există evaluări
- Clinical Approach To A Neonate With Cyanosis - Review - IJPDocument11 paginiClinical Approach To A Neonate With Cyanosis - Review - IJPSridhar KaushikÎncă nu există evaluări
- Infant of Diabetic Mother: DR: Eman Khammas Al-SadiDocument60 paginiInfant of Diabetic Mother: DR: Eman Khammas Al-SadiEman KhammasÎncă nu există evaluări
- Bladder Extrophy: Medical ManagementDocument8 paginiBladder Extrophy: Medical ManagementChristian James CamaongayÎncă nu există evaluări
- Duodenal ObstructionDocument53 paginiDuodenal ObstructionBoby ChandraÎncă nu există evaluări
- Hanan Fathy Pediatric Nephrology UnitDocument59 paginiHanan Fathy Pediatric Nephrology UnitdrhananfathyÎncă nu există evaluări
- 1 Fetal CirculationDocument23 pagini1 Fetal Circulationmohanad11Încă nu există evaluări
- Embryology-Nervous System DevelopmentDocument157 paginiEmbryology-Nervous System DevelopmentGheavita Chandra DewiÎncă nu există evaluări
- Fluid and Electrolyte Therapy - SeblewongelDocument47 paginiFluid and Electrolyte Therapy - SeblewongelSeblewongel AsemeÎncă nu există evaluări
- Neonatal Sepsis 1Document18 paginiNeonatal Sepsis 1Fãhâd Õró ÂhmédÎncă nu există evaluări
- #5 Neonatal Cardiac AnomaliesDocument93 pagini#5 Neonatal Cardiac AnomaliesSittie Hania100% (2)
- Hypoglycaemia FinalDocument31 paginiHypoglycaemia FinalJian Han LiewÎncă nu există evaluări
- Blood Transfusion in Pediatrics - Dr. RiniDocument55 paginiBlood Transfusion in Pediatrics - Dr. RiniAndyani PratiwiÎncă nu există evaluări
- Embryology Cardiovascula Rsystem DevelopmentDocument128 paginiEmbryology Cardiovascula Rsystem DevelopmentGhaidaa SadeqÎncă nu există evaluări
- Case Study #1: HistoryDocument39 paginiCase Study #1: Historyleonzon_ben442296Încă nu există evaluări
- Clinical Aspect of HyperbilirubinemiaDocument39 paginiClinical Aspect of HyperbilirubinemiaAfdelina RizkyÎncă nu există evaluări
- By: Jacqueline I. Esmundo, R.N.MNDocument32 paginiBy: Jacqueline I. Esmundo, R.N.MNdomlhynÎncă nu există evaluări
- Respiratory Distress Syndrome: Islamic University Nursing CollegeDocument21 paginiRespiratory Distress Syndrome: Islamic University Nursing Collegeyaumil agisnaÎncă nu există evaluări
- True Undescened TestesDocument42 paginiTrue Undescened TestesSahirÎncă nu există evaluări
- Fetal and Neonatal ArrhthmiasDocument59 paginiFetal and Neonatal ArrhthmiasRihab Hafiz Othman100% (1)
- Congenital Heart DiseaseDocument74 paginiCongenital Heart DiseaseKeith LajotÎncă nu există evaluări
- Curs Fetal Abdominal AnomaliesDocument137 paginiCurs Fetal Abdominal AnomaliesCristi SoareceÎncă nu există evaluări
- Normal NewbornDocument127 paginiNormal Newbornjanetwillams100% (3)
- NNJDocument20 paginiNNJLatifah AlsahaleyÎncă nu există evaluări
- K32 - Pathology of Bone (Dr. Dody)Document60 paginiK32 - Pathology of Bone (Dr. Dody)faris100% (1)
- Nelson's Hour - 58-60Document51 paginiNelson's Hour - 58-60Josselle Sempio CalientaÎncă nu există evaluări
- Birth AsphyxiaDocument16 paginiBirth Asphyxianurul nabillaÎncă nu există evaluări
- Neonatal JaundiceDocument72 paginiNeonatal JaundiceThya HakimÎncă nu există evaluări
- Neonatal ProceduresDocument74 paginiNeonatal ProceduresIbrahim Sabra100% (1)
- AsphyxiaDocument35 paginiAsphyxiaAna Cristina Montillano100% (1)
- Neonatal Transition: Training of The Trainers Neonatal ResuscitationDocument36 paginiNeonatal Transition: Training of The Trainers Neonatal ResuscitationmitaÎncă nu există evaluări
- Retinopathy of Prematurity: Aao ReadingDocument34 paginiRetinopathy of Prematurity: Aao ReadingUNHAS OphthalmologyÎncă nu există evaluări
- Care of Child Having Bladder Exstrophy and EpispadiasDocument3 paginiCare of Child Having Bladder Exstrophy and EpispadiasGarima ChaudharyÎncă nu există evaluări
- Cyanotic Congenital Heart DiseaseDocument50 paginiCyanotic Congenital Heart DiseaseSasi KumarÎncă nu există evaluări
- PERINATAL MORTALITY Kartik Sept 2020Document12 paginiPERINATAL MORTALITY Kartik Sept 2020Kartik KumarasamyÎncă nu există evaluări
- DMTM - NTC Online Acq - V001 NOV 2020 (Eng)Document18 paginiDMTM - NTC Online Acq - V001 NOV 2020 (Eng)Kartik KumarasamyÎncă nu există evaluări
- PERINATAL MORTALITY Kartik Sept 2020Document12 paginiPERINATAL MORTALITY Kartik Sept 2020Kartik KumarasamyÎncă nu există evaluări
- What Are The Key Challenges in Different Types of Main Qualitative Research?Document11 paginiWhat Are The Key Challenges in Different Types of Main Qualitative Research?Kartik KumarasamyÎncă nu există evaluări
- Lear N Fund Application Form: Personal Details of ApplicantDocument5 paginiLear N Fund Application Form: Personal Details of ApplicantKartik KumarasamyÎncă nu există evaluări
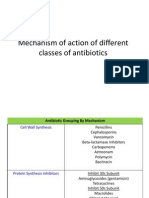
- Question 7 Mechanism of Action of Antibiotic Surgical Infection TBLDocument22 paginiQuestion 7 Mechanism of Action of Antibiotic Surgical Infection TBLKartik KumarasamyÎncă nu există evaluări
- What Is The Action of Heparin and What Would You Give To Counter Overdose of Heparin That Can Give A Life Threatening Bleed?Document1 paginăWhat Is The Action of Heparin and What Would You Give To Counter Overdose of Heparin That Can Give A Life Threatening Bleed?Kartik KumarasamyÎncă nu există evaluări
- Neonatal JaundiceDocument5 paginiNeonatal JaundiceKartik KumarasamyÎncă nu există evaluări
- Cold ChainDocument1 paginăCold ChainKartik KumarasamyÎncă nu există evaluări
- Mammalian HeartDocument7 paginiMammalian Heartnickmirad2Încă nu există evaluări
- An Introduction To Autopsy Technique: Step-by-Step DiagramsDocument24 paginiAn Introduction To Autopsy Technique: Step-by-Step Diagramskarin45Încă nu există evaluări
- Cardiovascular Physiology MCQsDocument24 paginiCardiovascular Physiology MCQsKlarens Affana63% (8)
- Suggested Answers To Practical Workbook: CH 7 Gas Exchange in HumansDocument31 paginiSuggested Answers To Practical Workbook: CH 7 Gas Exchange in HumansCharmine HolmesÎncă nu există evaluări
- AGT Applied Anatomy Notes1.1Document69 paginiAGT Applied Anatomy Notes1.1Akshay ChauhanÎncă nu există evaluări
- Cardiovascular EmbryologyDocument10 paginiCardiovascular EmbryologyChristianus LeonardÎncă nu există evaluări
- Embolization of Bronchial Arteries For The Treatment of HEMOPTYSIS. Update and Literature ReviewDocument20 paginiEmbolization of Bronchial Arteries For The Treatment of HEMOPTYSIS. Update and Literature ReviewHai SheikhÎncă nu există evaluări
- Surgery PackratDocument46 paginiSurgery PackratRicardo Nelson100% (4)
- Aortic DissectionDocument5 paginiAortic DissectionCosminNGDNÎncă nu există evaluări
- Thoraco AbdominalDocument8 paginiThoraco Abdominalamelia kartikaÎncă nu există evaluări
- CVS HistologyDocument43 paginiCVS Histologyبراءة أحمد السلامات100% (1)
- Abdominal Aortic Aneurysm Case Study: by Lisa ErwertDocument21 paginiAbdominal Aortic Aneurysm Case Study: by Lisa ErwertShashidhar Venkatesh MurthyÎncă nu există evaluări
- Nursing Practice 2-Pre-Board Examination-Vmuf.-College of Nursing - Revalida 2021Document55 paginiNursing Practice 2-Pre-Board Examination-Vmuf.-College of Nursing - Revalida 2021Dyanne BautistaÎncă nu există evaluări
- 8940Document166 pagini8940Basory Ok OkÎncă nu există evaluări
- Gel Polish and Dry Manicure Manual EDITABLEDocument56 paginiGel Polish and Dry Manicure Manual EDITABLECristina Gradinari100% (1)
- Topnotch Practice Exam 1 For MARCH 2020 and SEPT 2020 BatchesDocument104 paginiTopnotch Practice Exam 1 For MARCH 2020 and SEPT 2020 BatchesJerome AndresÎncă nu există evaluări
- Pediatric Patent Ductus ArteriosusDocument12 paginiPediatric Patent Ductus Arteriosusabirami_murugesuÎncă nu există evaluări
- Chest Trauma and Indication For ThoracotomyDocument57 paginiChest Trauma and Indication For ThoracotomydemmonÎncă nu există evaluări
- Housing and Maintenance of Ambystoma Mexicanum, The Mexican AxolotlDocument20 paginiHousing and Maintenance of Ambystoma Mexicanum, The Mexican AxolotlAngela HurtadoÎncă nu există evaluări
- AP WindowDocument13 paginiAP WindowHugo GonzálezÎncă nu există evaluări
- 0610 w14 QP 32Document24 pagini0610 w14 QP 32Haider AliÎncă nu există evaluări
- The Cardiovascular Centre Is A Part of The Human Brain Responsible For The Regulation of The Rate at Which The Heart BeatsDocument40 paginiThe Cardiovascular Centre Is A Part of The Human Brain Responsible For The Regulation of The Rate at Which The Heart BeatsNeha Sharma100% (2)
- The Most CommonsDocument80 paginiThe Most CommonsJmee8Încă nu există evaluări
- MCQS, Emryology of The HeartDocument22 paginiMCQS, Emryology of The HeartERIAS TENYWAÎncă nu există evaluări
- Aortic SurgeryDocument355 paginiAortic SurgeryPaola Rojas GuevaraÎncă nu există evaluări
- Congenital Anomalies: Pooja K MenonDocument73 paginiCongenital Anomalies: Pooja K Menonpujitha2002100% (2)
- 7mm Frog ATLAS 2Document28 pagini7mm Frog ATLAS 2aemilianneÎncă nu există evaluări
- AbdomenDocument2 paginiAbdomenRhea Rose Turno - N1EÎncă nu există evaluări
- The Circulatory System (Cardiovascular System) Pumps Blood From TheDocument6 paginiThe Circulatory System (Cardiovascular System) Pumps Blood From ThevanÎncă nu există evaluări
- New Contruncal DevelopmentDocument66 paginiNew Contruncal DevelopmentMarian AlexÎncă nu există evaluări