S-ar putea să vă placă și
- Grand Case PresentationDocument28 paginiGrand Case PresentationRae Marie AquinoÎncă nu există evaluări
- Kainat KhanDocument39 paginiKainat Khanabeehaarshad113Încă nu există evaluări
- Case PresentationDocument21 paginiCase PresentationMae Alleslie TolentinoÎncă nu există evaluări
- Bipolar Mood DisorderDocument30 paginiBipolar Mood DisorderJohn Patrick Macasasa100% (2)
- Schizophrenia NCMH Case StudyDocument45 paginiSchizophrenia NCMH Case StudyHomework PingÎncă nu există evaluări
- Undifferentiated SchizophreniaDocument47 paginiUndifferentiated SchizophreniaChezka Palola100% (1)
- Schizophrenia Case StudyDocument24 paginiSchizophrenia Case StudyRichard Sy100% (3)
- Case Presentation SchizoDocument13 paginiCase Presentation SchizoBarbara Detaro100% (1)
- Case Study On PARANOID SCHIZOPHRENIA Melisa 19Document29 paginiCase Study On PARANOID SCHIZOPHRENIA Melisa 19MELISA ELEUTHEREÎncă nu există evaluări
- EricDocument46 paginiEricandrea villanuevaÎncă nu există evaluări
- Schizophrenia NCMH Case StudyDocument45 paginiSchizophrenia NCMH Case StudyNickale Peralta100% (1)
- Case Study MH ClinicalDocument10 paginiCase Study MH Clinicalapi-546401036Încă nu există evaluări
- Mental Health Case StudyDocument11 paginiMental Health Case Studyapi-607361848Încă nu există evaluări
- Case PresentationDocument2 paginiCase Presentationapi-263066835Încă nu există evaluări
- Case No 2 SchizoDocument8 paginiCase No 2 SchizoSarah Saqib AhmadÎncă nu există evaluări
- Counselling Psychology SeminarDocument6 paginiCounselling Psychology Seminarmadhu mithaÎncă nu există evaluări
- ASIM Issue 4 10Dp904 907 PDFDocument4 paginiASIM Issue 4 10Dp904 907 PDFadeÎncă nu există evaluări
- Psychiatric Mental Health Comprehensive Case StudyDocument12 paginiPsychiatric Mental Health Comprehensive Case Studyapi-496883420Încă nu există evaluări
- Case Study: Anna Liza CorpuzDocument72 paginiCase Study: Anna Liza CorpuzAnna Liza Adon CorpuzÎncă nu există evaluări
- Case Study BipolarDocument22 paginiCase Study BipolarRobert de Guzman Jr.93% (29)
- Psychiatric Case PresentationDocument73 paginiPsychiatric Case PresentationRechie Gallo50% (2)
- FiNAL CASE.Document50 paginiFiNAL CASE.John CrisostomoÎncă nu există evaluări
- Psycology Project........ Case Study and MisconceotonsDocument12 paginiPsycology Project........ Case Study and Misconceotonscom22730Încă nu există evaluări
- A Layperson's Guide to Living with Mental DiseaseDe la EverandA Layperson's Guide to Living with Mental DiseaseÎncă nu există evaluări
- Student Name Institution Professor Course DateDocument9 paginiStudent Name Institution Professor Course DatefestusÎncă nu există evaluări
- CasestudyDocument12 paginiCasestudyapi-354053517Încă nu există evaluări
- Mental Health Case StudyDocument12 paginiMental Health Case Studyapi-603542802Încă nu există evaluări
- Bataan Case EditedDocument21 paginiBataan Case EditedCham Rafaela ConeseÎncă nu există evaluări
- New Case StudyDocument15 paginiNew Case Studyapi-507336246Încă nu există evaluări
- Internship ReportDocument16 paginiInternship ReportRACHANA MURALIDHAR 1833279Încă nu există evaluări
- 1.A Ndera CaseDocument13 pagini1.A Ndera CaseNsengimana Eric MaxigyÎncă nu există evaluări
- Case PresantationDocument15 paginiCase PresantationHezron BihogoraÎncă nu există evaluări
- Case StudyDocument9 paginiCase Studyapsari.mhiÎncă nu există evaluări
- Michael Kilfoyle - Centrelink DSP Support Letter 09072019 2Document3 paginiMichael Kilfoyle - Centrelink DSP Support Letter 09072019 2mkilfoyle11Încă nu există evaluări
- Case Report: JR: Melissa Leviste and Nami MuzoDocument28 paginiCase Report: JR: Melissa Leviste and Nami MuzoNami MuzoÎncă nu există evaluări
- Psych Case StudyDocument32 paginiPsych Case StudyAndrea Isabel U. O'DellÎncă nu există evaluări
- OK - HP8003 NotesDocument71 paginiOK - HP8003 NotesjamesngÎncă nu există evaluări
- Psychiatric Report: Psychiatric Exam I. General DataDocument4 paginiPsychiatric Report: Psychiatric Exam I. General DataCourtneyÎncă nu există evaluări
- B. Bipolar Disorder, Manic EpisodeDocument7 paginiB. Bipolar Disorder, Manic EpisodeJeisson EspinelÎncă nu există evaluări
- Paranoid SchizophreniaDocument21 paginiParanoid SchizophreniaRizwan ZafarÎncă nu există evaluări
- Case ReportDocument13 paginiCase ReportZaryab Waheed0% (1)
- Kleinberger Depression in Infancy-1Document4 paginiKleinberger Depression in Infancy-1Felipe Marín BahamondesÎncă nu există evaluări
- Elective Mutism: A Case Study: KeywordsDocument3 paginiElective Mutism: A Case Study: KeywordsMartinis de las MercedesÎncă nu există evaluări
- Case Study PsychDocument49 paginiCase Study PsychMonique Reyes100% (1)
- Bipolar DisorderDocument48 paginiBipolar DisorderRey Jayvee Arcuino Hinunangan50% (2)
- PsychosisDocument5 paginiPsychosisRalph Lorenz Avila AquinoÎncă nu există evaluări
- Case Analysis in Psych Bipolar Disorder BYDocument13 paginiCase Analysis in Psych Bipolar Disorder BYSheryl Ann Barit PedinesÎncă nu există evaluări
- CASE Presentation Psychia Holy Child College of DavaoDocument45 paginiCASE Presentation Psychia Holy Child College of DavaoMonemah Essa Francisco Martinez100% (2)
- PSYCHreportDocument4 paginiPSYCHreportjoyce ramirezÎncă nu există evaluări
- Dissociative DisordersDocument25 paginiDissociative DisordersKholoud KholoudÎncă nu există evaluări
- Cases from the Psychiatry Letter - I: Cases from the Psychiatry Letter, #1De la EverandCases from the Psychiatry Letter - I: Cases from the Psychiatry Letter, #1Evaluare: 5 din 5 stele5/5 (1)
- Kursus Kompetensi Intervensi KPM 040723Document45 paginiKursus Kompetensi Intervensi KPM 040723FILBERT ANAK HAGAR KPM-GuruÎncă nu există evaluări
- Shared Psychotic Disorder A Case Study Submitted byDocument27 paginiShared Psychotic Disorder A Case Study Submitted byChin Lee100% (1)
- In Search of Madness: A Psychiatrist's Travels Through the History of Mental IllnessDe la EverandIn Search of Madness: A Psychiatrist's Travels Through the History of Mental IllnessÎncă nu există evaluări
- Deepa SekharDocument4 paginiDeepa SekharThakur Manu PratapÎncă nu există evaluări
- Bipolar Disorder Case Study 1Document15 paginiBipolar Disorder Case Study 1api-662433822Încă nu există evaluări
- Psychiatric Diagnoses and Psychological Test ResultsDocument21 paginiPsychiatric Diagnoses and Psychological Test ResultsGary FreedmanÎncă nu există evaluări
- Comprehensive Case StudyDocument11 paginiComprehensive Case Studyapi-546503916Încă nu există evaluări
- Case Analysis SchizoDocument4 paginiCase Analysis SchizoiamELHIZAÎncă nu există evaluări
- Bone Healing StagesDocument2 paginiBone Healing StagesSean TecsonÎncă nu există evaluări
- Hyperthermia NCPDocument3 paginiHyperthermia NCPSean TecsonÎncă nu există evaluări
- MethergineDocument2 paginiMethergineSean TecsonÎncă nu există evaluări
- MethergineDocument2 paginiMethergineSean TecsonÎncă nu există evaluări
- Substitution Table ExplainedDocument7 paginiSubstitution Table ExplainedaimarÎncă nu există evaluări
- Evandro Agazzi - Philosophy and The Origin and Evolution of The UniverseDocument472 paginiEvandro Agazzi - Philosophy and The Origin and Evolution of The UniverseSettemontiErma1100% (1)
- PSYC 101 002 SyllabusDocument6 paginiPSYC 101 002 Syllabusamolapf4Încă nu există evaluări
- RUBRIC Topic - Project Defense1Document3 paginiRUBRIC Topic - Project Defense1Ar JCÎncă nu există evaluări
- Girl Scouts of The Philippines Action PlanDocument3 paginiGirl Scouts of The Philippines Action PlanRd DavidÎncă nu există evaluări
- Project Report On Competency MappingDocument22 paginiProject Report On Competency MappingJayesh Gaonkar100% (2)
- Tutorials /assignments: Aditya Silver Oak Institute of TechnologyDocument9 paginiTutorials /assignments: Aditya Silver Oak Institute of TechnologyDipika GuptaÎncă nu există evaluări
- Partition AgreementDocument4 paginiPartition AgreementFulgue Joel67% (12)
- English Essay About Indonesia's Education ProgramDocument2 paginiEnglish Essay About Indonesia's Education ProgramDesratri Timur TresnantiÎncă nu există evaluări
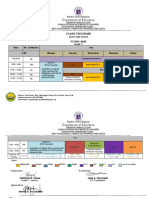
- Class Program Grade 7-10Document9 paginiClass Program Grade 7-10jake felicianoÎncă nu există evaluări
- Introductory Exhibit LabelsDocument3 paginiIntroductory Exhibit LabelsSteven LubarÎncă nu există evaluări
- Certificate Resource SpeakerDocument5 paginiCertificate Resource SpeakerAbegail H. Laquiao78% (9)
- Redefining The Role of The TeacherDocument4 paginiRedefining The Role of The TeacherJavier DominguezÎncă nu există evaluări
- Basic Punjabi - Lesson 3 - Introducing Yourself and FamilyDocument34 paginiBasic Punjabi - Lesson 3 - Introducing Yourself and FamilyCulture AlleyÎncă nu există evaluări
- (CO Validation) Enclosure No. 2 - School Readiness ChecklistDocument1 pagină(CO Validation) Enclosure No. 2 - School Readiness ChecklistBryan MoyaÎncă nu există evaluări
- Ghelay Application LetterDocument4 paginiGhelay Application LetterMonica JavierÎncă nu există evaluări
- Transactional AnalysisDocument31 paginiTransactional AnalysisCostel PopÎncă nu există evaluări
- Use of Sim (Strategic Intervention Material) As Strategy and The Academic Achievement of Grade 7 Students On Selected Topic in Earth ScienceDocument11 paginiUse of Sim (Strategic Intervention Material) As Strategy and The Academic Achievement of Grade 7 Students On Selected Topic in Earth ScienceGlobal Research and Development ServicesÎncă nu există evaluări
- Bluebook Abbreviations of Law Reviews & Legal Periodicals Indexed in CILPDocument20 paginiBluebook Abbreviations of Law Reviews & Legal Periodicals Indexed in CILPRicharnellia-RichieRichBattiest-CollinsÎncă nu există evaluări
- Emergency Care SopsDocument12 paginiEmergency Care SopsMA.RESA M.GALIDOÎncă nu există evaluări
- Pblhndbk2009 Queen's UniversityDocument32 paginiPblhndbk2009 Queen's UniversityAziz JamaludinÎncă nu există evaluări
- Critical Thinking Skills For Leadership DevelopmentDocument12 paginiCritical Thinking Skills For Leadership Developmentdali77Încă nu există evaluări
- Veda Vyasa D.A.V. Public SchoolDocument1 paginăVeda Vyasa D.A.V. Public SchoolDivyansh SharmaÎncă nu există evaluări
- Pro and Anti K-12Document1 paginăPro and Anti K-12Marianel Antiqueña EspinosaÎncă nu există evaluări
- t2tt Training Modules - CompressedDocument335 paginit2tt Training Modules - CompressedNaina MalikÎncă nu există evaluări
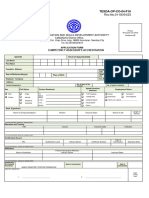
- Updated Assessors' Application FormDocument1 paginăUpdated Assessors' Application FormLieza MarianoÎncă nu există evaluări
- Lect. 6.2 Caribbean EducationDocument8 paginiLect. 6.2 Caribbean EducationToriÎncă nu există evaluări
- Science and Its TimesDocument512 paginiScience and Its Timesluis peixotoÎncă nu există evaluări
- 9 - 12thDocument2 pagini9 - 12thapi-336834578Încă nu există evaluări
- Mathematical ModelingDocument3 paginiMathematical ModelingJunyipp ChaiÎncă nu există evaluări