S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Risk Criteria - When Is Low Enough Good Enough - SaudiDocument8 paginiRisk Criteria - When Is Low Enough Good Enough - Saudiuserscribd2011Încă nu există evaluări
- Seismic Aspects of Dam Design PDFDocument12 paginiSeismic Aspects of Dam Design PDFAlokÎncă nu există evaluări
- AripiprazoleDocument2 paginiAripiprazoleKrisianne Mae Lorenzo FranciscoÎncă nu există evaluări
- Selecting A Sulfonylurea: Pharmacist'S Letter / Prescriber'S LetterDocument3 paginiSelecting A Sulfonylurea: Pharmacist'S Letter / Prescriber'S Lettercarramrod2Încă nu există evaluări
- Comparison of Common Meds For Diabetic Neuropathy: Pharmacist'S Letter / Prescriber'S LetterDocument5 paginiComparison of Common Meds For Diabetic Neuropathy: Pharmacist'S Letter / Prescriber'S Lettercarramrod2Încă nu există evaluări
- 1215Document11 pagini1215carramrod2Încă nu există evaluări
- 250803111111Document4 pagini250803111111carramrod2Încă nu există evaluări
- 1214Document4 pagini1214carramrod2Încă nu există evaluări
- Initiation and Adjustment of Insulin Regimens For Type 2 DiabetesDocument2 paginiInitiation and Adjustment of Insulin Regimens For Type 2 Diabetescarramrod2Încă nu există evaluări
- 1253Document3 pagini1253carramrod2Încă nu există evaluări
- Thiazides and Diabetes: Pharmacist'S Letter / Prescriber'S LetterDocument2 paginiThiazides and Diabetes: Pharmacist'S Letter / Prescriber'S Lettercarramrod2Încă nu există evaluări
- 205rfqergqergDocument4 pagini205rfqergqergcarramrod2Încă nu există evaluări
- DfsefDocument4 paginiDfsefcarramrod2Încă nu există evaluări
- Treatment of Diabetes in Women Who Are Pregnant: Pharmacist'S Letter / Prescriber'S LetterDocument5 paginiTreatment of Diabetes in Women Who Are Pregnant: Pharmacist'S Letter / Prescriber'S Lettercarramrod2Încă nu există evaluări
- 1107Document5 pagini1107carramrod2Încă nu există evaluări
- Proper Disposal of Expired or Unwanted DrugsDocument9 paginiProper Disposal of Expired or Unwanted Drugscarramrod2Încă nu există evaluări
- 3807Document2 pagini3807carramrod2Încă nu există evaluări
- Prescribing For Self or FamilyDocument15 paginiPrescribing For Self or Familycarramrod2100% (2)
- Tablet Splitting - To Split or Not To SplitDocument2 paginiTablet Splitting - To Split or Not To Splitcarramrod2Încă nu există evaluări
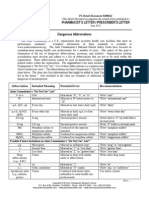
- Dangerous AbbreviationsDocument3 paginiDangerous Abbreviationscarramrod2Încă nu există evaluări
- Management of Common Skin DiseasesDocument17 paginiManagement of Common Skin Diseasescarramrod2Încă nu există evaluări
- NSTP 2 Modules Lesson on Community OrganizingDocument14 paginiNSTP 2 Modules Lesson on Community OrganizingJestony Riray CagmatÎncă nu există evaluări
- Engineering Properties of Soil PDFDocument55 paginiEngineering Properties of Soil PDFJam Apizara Chaizalee100% (1)
- MC Data Dig Graphic Organizer 1Document5 paginiMC Data Dig Graphic Organizer 1api-461486414Încă nu există evaluări
- Princes of the Apocalypse Locations IndexDocument2 paginiPrinces of the Apocalypse Locations IndexPedroManzelaDuarteÎncă nu există evaluări
- HR Syl 5 Pages 2023-2024 20.09.2023Document5 paginiHR Syl 5 Pages 2023-2024 20.09.2023ABLEELECTRONÎncă nu există evaluări
- ''Let All God's Angels Worship Him'' - Gordon AllanDocument8 pagini''Let All God's Angels Worship Him'' - Gordon AllanRubem_CLÎncă nu există evaluări
- 4 03 02 Iep and Lesson Plan Development Handbook - Schoolhouse DocumentDocument42 pagini4 03 02 Iep and Lesson Plan Development Handbook - Schoolhouse Documentapi-252552726Încă nu există evaluări
- Technical and Cost Model For Slipway DevelopmentDocument36 paginiTechnical and Cost Model For Slipway DevelopmentshahjadaÎncă nu există evaluări
- GEY 102-Introduction To Geology 1-Lecture Slides - Prof. M.E. NtonDocument44 paginiGEY 102-Introduction To Geology 1-Lecture Slides - Prof. M.E. Ntonabuabdmuqseet2001Încă nu există evaluări
- Agenda For Regular Board Meeting February 18, 2022 Western Visayas Cacao Agriculture CooperativeDocument2 paginiAgenda For Regular Board Meeting February 18, 2022 Western Visayas Cacao Agriculture CooperativeGem Bhrian IgnacioÎncă nu există evaluări
- 50 Sets of Puzzles and Seating Arrangement For IBPS PO Mains 2017 SolutionsDocument23 pagini50 Sets of Puzzles and Seating Arrangement For IBPS PO Mains 2017 SolutionssaÎncă nu există evaluări
- 50 Important Quotes You Should Pay Attention To in Past The Shallows Art of Smart EducationDocument12 pagini50 Important Quotes You Should Pay Attention To in Past The Shallows Art of Smart EducationSailesh VeluriÎncă nu există evaluări
- Vaclav Havel - From 'Mistake'. SAGEDocument9 paginiVaclav Havel - From 'Mistake'. SAGEADIELruleÎncă nu există evaluări
- Lower and Upper Bound Theory ExplainedDocument37 paginiLower and Upper Bound Theory ExplainedTsuki ZombinaÎncă nu există evaluări
- Making Hand Sanitizer from Carambola FruitDocument5 paginiMaking Hand Sanitizer from Carambola FruitMary grace LlagasÎncă nu există evaluări
- Misrepresentation by Non-Disclosure in South African Law 2013Document163 paginiMisrepresentation by Non-Disclosure in South African Law 2013Faiez KirstenÎncă nu există evaluări
- Progressivism Lesson 3 The PresidentsDocument3 paginiProgressivism Lesson 3 The Presidentsapi-302923213Încă nu există evaluări
- SLI ProfileThe title "TITLE SLI Profile" is less than 40 characters and starts with "TITLEDocument3 paginiSLI ProfileThe title "TITLE SLI Profile" is less than 40 characters and starts with "TITLEcringeÎncă nu există evaluări
- Flyposting OrdinanceDocument2 paginiFlyposting OrdinanceJunil LagardeÎncă nu există evaluări
- Depository Receipts: Presented By-Vikash Sharma (51) Ruchi BangaDocument12 paginiDepository Receipts: Presented By-Vikash Sharma (51) Ruchi Bangasuraj kumar0% (1)
- Sap Interface PDFDocument1 paginăSap Interface PDFAwais SafdarÎncă nu există evaluări
- Dreams PDFDocument8 paginiDreams PDFapi-266967947Încă nu există evaluări
- Reading at the BeachDocument3 paginiReading at the BeachhihiijklkoÎncă nu există evaluări
- MSO 1st Year Assignments 2017-18 (English) PDFDocument7 paginiMSO 1st Year Assignments 2017-18 (English) PDFAmritpal BhagatÎncă nu există evaluări
- Crafting Your Keto Diet MindsetDocument3 paginiCrafting Your Keto Diet MindsetoculosoakleyÎncă nu există evaluări
- Physics 5th Edition Walker Test BankDocument24 paginiPhysics 5th Edition Walker Test BankKathyHernandeznobt100% (31)
- A History Analysis and Performance Guide To Samuel Barber?Document117 paginiA History Analysis and Performance Guide To Samuel Barber?giorgio planesioÎncă nu există evaluări