S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Yes We CanDocument1 paginăYes We CanfrakturhepatikaÎncă nu există evaluări
- We GotDocument1 paginăWe GotfrakturhepatikaÎncă nu există evaluări
- Present As IDocument1 paginăPresent As IfrakturhepatikaÎncă nu există evaluări
- Oke BismillahDocument1 paginăOke BismillahfrakturhepatikaÎncă nu există evaluări
- G6PD Deficiency Prevalence and Estimates of Affected Populations in Malaria Endemic Countries: A Geostatistical Model-Based MapDocument101 paginiG6PD Deficiency Prevalence and Estimates of Affected Populations in Malaria Endemic Countries: A Geostatistical Model-Based MapfrakturhepatikaÎncă nu există evaluări
- Mah Sakirt RSIDocument1 paginăMah Sakirt RSIfrakturhepatikaÎncă nu există evaluări
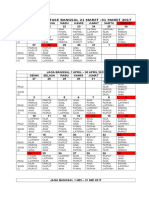
- Jadwal Jaga Stase Bangsal 21 Maret - 31 Maret 2017Document4 paginiJadwal Jaga Stase Bangsal 21 Maret - 31 Maret 2017frakturhepatikaÎncă nu există evaluări
- Anestesi JurnalDocument10 paginiAnestesi JurnalfrakturhepatikaÎncă nu există evaluări
- Out 551Document10 paginiOut 551frakturhepatikaÎncă nu există evaluări
- TugasDocument4 paginiTugasfrakturhepatikaÎncă nu există evaluări
- Albumin Versus Other Fluids For Fluid Resuscitation in Patients With Sepsis: A Meta-AnalysisDocument22 paginiAlbumin Versus Other Fluids For Fluid Resuscitation in Patients With Sepsis: A Meta-AnalysisfrakturhepatikaÎncă nu există evaluări
- Guidance For Intravenous Fluid and Electrolyte Prescription in AdultsDocument8 paginiGuidance For Intravenous Fluid and Electrolyte Prescription in AdultsfrakturhepatikaÎncă nu există evaluări
- Basic and Advanced Cardiac Life Support: What's New?Document6 paginiBasic and Advanced Cardiac Life Support: What's New?frakturhepatikaÎncă nu există evaluări
- Fluid Resuscitation in Acute Illness - Time To Reappraise The BasicsDocument2 paginiFluid Resuscitation in Acute Illness - Time To Reappraise The BasicsAlina AndreiÎncă nu există evaluări
- S0149291812X00031 S0149291812001695 MainDocument1 paginăS0149291812X00031 S0149291812001695 MainfrakturhepatikaÎncă nu există evaluări
- Risk Factors For Chronic and Recurrent Otitis Media-A Meta-AnalysisDocument9 paginiRisk Factors For Chronic and Recurrent Otitis Media-A Meta-AnalysisNadhira Puspita AyuningtyasÎncă nu există evaluări
- Pediatric Rehabilitation FiDocument61 paginiPediatric Rehabilitation FifrakturhepatikaÎncă nu există evaluări
- Evaluation of Paracetamol Distribution and Stability in Case of Acute Intoxication in Rats - ProQuest - 2Document9 paginiEvaluation of Paracetamol Distribution and Stability in Case of Acute Intoxication in Rats - ProQuest - 2frakturhepatikaÎncă nu există evaluări
- ObatDocument3 paginiObatfrakturhepatikaÎncă nu există evaluări
- Sri MurtiniDocument15 paginiSri MurtiniRatno AriyansahÎncă nu există evaluări
- Aku BisaDocument13 paginiAku BisafrakturhepatikaÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- DR. ARIFIN - CAP (New PDPI Guideline)Document36 paginiDR. ARIFIN - CAP (New PDPI Guideline)Inggriht Senny BondangÎncă nu există evaluări
- SIP 2016 Abstract & Background Booklet V.6 PDFDocument187 paginiSIP 2016 Abstract & Background Booklet V.6 PDFJimboreanu György PaulaÎncă nu există evaluări
- Lipid Metabolism and Health - EBOOKOID PDFDocument377 paginiLipid Metabolism and Health - EBOOKOID PDFniluh suwasantiÎncă nu există evaluări
- Diagnosis Holistik Kedokteran Keluarga PPT - Ulfi Nela YanarDocument43 paginiDiagnosis Holistik Kedokteran Keluarga PPT - Ulfi Nela YanarUlfiYanarÎncă nu există evaluări
- Introduction To Waterborne PathogensDocument60 paginiIntroduction To Waterborne PathogensSyed Alwi Alattas100% (1)
- Human Behavior and Crisis Management (Bigwas)Document3 paginiHuman Behavior and Crisis Management (Bigwas)Randal's CaseÎncă nu există evaluări
- Renal and Urinary SystemDocument5 paginiRenal and Urinary SystemStaceyÎncă nu există evaluări
- Hema LecDocument20 paginiHema LecJOWELA RUBY EUSEBIOÎncă nu există evaluări
- EpiDocument3 paginiEpiNiño PaoloÎncă nu există evaluări
- Rheumatic Heart DiseaseDocument4 paginiRheumatic Heart DiseaseAlfrin Antony100% (3)
- The Garage Built Body Main Program GuideDocument21 paginiThe Garage Built Body Main Program GuideNoel Martin100% (1)
- Daun PDFDocument5 paginiDaun PDFDaniel OktavianusÎncă nu există evaluări
- 079 Muhammad Khairul Nizam Bin Khir 7.1Document30 pagini079 Muhammad Khairul Nizam Bin Khir 7.1Ilham RafisÎncă nu există evaluări
- Bertram Georgette EuniceDocument4 paginiBertram Georgette EuniceArabela SimbahanÎncă nu există evaluări
- Summary of Anxiety Disorders (DSM-5)Document6 paginiSummary of Anxiety Disorders (DSM-5)Villamorchard100% (3)
- Pursed Lips Breathing and CHFDocument6 paginiPursed Lips Breathing and CHFErwan HermansyahÎncă nu există evaluări
- Complete Health HistoryDocument22 paginiComplete Health HistorykhalidÎncă nu există evaluări
- Biology Investigatory Project: Topic: Parkinson'S DiseaseDocument18 paginiBiology Investigatory Project: Topic: Parkinson'S DiseaseAneesh MoosaÎncă nu există evaluări
- The Cornell Scale For Depression in DementiaDocument12 paginiThe Cornell Scale For Depression in DementiaPopa NiculinaÎncă nu există evaluări
- Finney Ms Case StudyDocument17 paginiFinney Ms Case Studyapi-255767391Încă nu există evaluări
- BHP Formula No 55 Refrence - Aesculus Pentarkan PTK 3 Best Homeopathic Medicine For PilesDocument3 paginiBHP Formula No 55 Refrence - Aesculus Pentarkan PTK 3 Best Homeopathic Medicine For PilesKazy Habibur RahmanÎncă nu există evaluări
- EpidemiologyDocument32 paginiEpidemiologyIshika RoyÎncă nu există evaluări
- QuizDocument8 paginiQuizJohara Mae De RamaÎncă nu există evaluări
- Quiz RespiratoryDocument123 paginiQuiz RespiratoryMedShare100% (23)
- Nursing Care Plan Assessment Planning Intervention Rationale Expected OutcomeDocument4 paginiNursing Care Plan Assessment Planning Intervention Rationale Expected OutcomeAshley Kate SantosÎncă nu există evaluări
- Online NUrsing Exam Question AnswersDocument2 paginiOnline NUrsing Exam Question AnswersCandra P100% (3)
- Risk Managemnt ReviewerDocument4 paginiRisk Managemnt ReviewerHaru CutieÎncă nu există evaluări
- Q A 1Document48 paginiQ A 1ChannelGÎncă nu există evaluări
- Cestosis y Cestodos PDFDocument14 paginiCestosis y Cestodos PDFErnesto VersailleÎncă nu există evaluări
- An Effective Simple Treatment of Perichondritis and Haematoma of PinnaDocument10 paginiAn Effective Simple Treatment of Perichondritis and Haematoma of Pinnaputri hidayah afrianiÎncă nu există evaluări