Documente Academic
Documente Profesional
Documente Cultură
PhysicianJanuary February12 PDF
Încărcat de
CostelloforCongressDescriere originală:
Titlu original
Drepturi de autor
Formate disponibile
Partajați acest document
Partajați sau inserați document
Vi se pare util acest document?
Este necorespunzător acest conținut?
Raportați acest documentDrepturi de autor:
Formate disponibile
PhysicianJanuary February12 PDF
Încărcat de
CostelloforCongressDrepturi de autor:
Formate disponibile
Physician
January/February 2012
vol. 18, no. 1
News for Medical Staff, Residents, Fellows and Alumni
MEDSTAR WASHINGTON HOSPITAL CENTER
MedStar Health Rebranding:
Coming Together
Under One Name
Inside
3
Using ECMO,
Saving a Life
4
Cover Story
9
"State of the
Heart"
10
New Horizon
for Cancer
Care
3
JAN/FEB 2012 | PHYSICIAN | MEDSTAR WASHINGTON HOSPITAL CENTER
3
Picture a concert violinist, with his
instrument and bow.
If his goal is to expertly play the violin, each element is vital. Take
away an element, say, the bow, and he cant reach his goal.
Lets use that image of the concert violinist, with our goal of always
striving to increase physician engagement.
Physicians here are the bow that is crucial to the success of MedStar
Washington Hospital Center as a High Reliability Organization
(HRO), as embraced by the Agency for Healthcare Research and
Quality (AHRQ).
Youve shared your concerns, and we have been working on all the
issues youve brought up in previous surveys. Many of you took the
physician engagement survey last fall, and have been involved in the
processes to change your areas of concern. Thank you for letting us
know youve noticed differences for some of those areas. You told us
in the most recent survey:
n The Hospital Center is actively working to improve patient safety,
and you are satisfied with the continuity of care you can provide
your patients.
n You enjoy both working with other faculty in your department
and the level of collegiality you all share. You feel teaching
residents is a priority for your professional development, and that
there is both a reasonable teaching schedule and student/faculty
ratio.
n You are satisfied with the accuracy of results and key information
from the Emergency Department, Radiology and Laboratory
Services.
n You like the availability of continuing medical education (CME)
available to you.
n You believe the hospital administration treats physicians with
respect, and you would recommend the Hospital Center as a
good place to practice medicine.
n You would recommend the Hospital Center to family and friends
who need care.
With your help, here are the additional areas we will focus on to
increase your level of engagement at the hospital. We will work
together to:
n Ease the registration and scheduling process for your patients,
and improve the efficiency of patient flow and the completion of
paperwork,
n Continue to improve the appearance and cleanliness in patient
care areas,
n Form stronger teams with our Nursing colleagues, to provide
compassionate care, responsiveness and expertise at the bedside.
The action plans to address more specific concerns will be addressed
by a committee that will be charged with developing overall action
plans for the survey. In addition, in each department
interdisciplinary groups will be brought together by your
department chair. Everyone will be asked to regularly assess the
success of the plans and revise them, as needed.
The new tagline for MedStar Health sums up what we are promising
to our patients, their families and our communities: Knowledge
and Compassion, Focused on You.
We can all help show that we live that tagline, by personally making a
difference every day. I encourage all of you to become more involved
with your departments. The system of providing health care in
America continues to evolve. We need your input and new ways of
thinking outside the box, to inspire creative and innovative
approaches to problem-solving.
Thank you for your continuing support for the Hospital Center.
Janis M. Orlowski, MD, MACP, is senior vice president, Medical Affairs
and Chief Medical Officer at MedStar Washington Hospital Center. She
can be reached at 202-877-5284 and via email,
janis.m.orlowski@medstar.net.
2 MEDSTAR WASHINGTON HOSPITAL CENTER | PHYSICIAN | JAN/FEB 2012 2
C H I E F ME D I C A L O F F I C E R
Rare Combination Therapy Gives
Burn Patient Second Chance at Life
The patient was dying, and her doctors were
running out of ways to prevent it.
Less than a week earlier, the Washington area woman had been
enjoying a friends backyard cookout when a firepot exploded,
spraying her with hot citronella fuel. She was rushed to The Burn
Center at MedStar Washington Hospital Center, with mostly
third-degree burns over 50 percent of her body, and smoke
inhalation. Now, she had developed hospital-acquired pneumonia
(HAP), a common occurrence for patients on ventilators.
Though HAP is usually controllable, this patients case was
accelerating rapidlyto the point where her lungs were on verge of
irreversible failure.
We attempted all the
conventional ventilation
treatments, none of which
improved her condition, recalls
James C. Jeng, MD, associate
director of The Burn Center.
Under any other circumstances,
she would have just died.
But she had one thing in her
favor: the close availability of a
technology called extracorporeal
membrane oxygenation, or
ECMO.
Similar to other types of
heart/lung machines, ECMO
temporarily takes over the processing of blood and oxygen from
damaged cardiac and respiratory systems, allowing lungs and other
organs to heal.
ECMO is hardly a go-to treatment, however, as its use is generally
limited to full-term newborn infants with virus infections or defective
respiratory systems, and only then as a last resort.
Dr. Jeng explains that applications of ECMO for adult patients are
rare and a little controversial, given the historically high risk of
neurological injury, infection and internal bleeding.
Much of the time, ECMO is contraindicated in adults, because it
complicates what is already a highly intricate mix of treatments,
particularly for burn victims, he says. However, we are finding that
in select cases, ECMO can be used successfully.
In Dr. Jengs opinion, this was one of those cases. Indeed, using
ECMO was likely the patients last hope for survival.
Fortunately, ECMO equipment and the team of experts needed to use
it were available almost literally next door, at the Hospital Centers
Surgical Intensive Care unit.
Its rare that you have the combination of burn treatment and
ECMO technology at the same facility, Dr. Jeng says. Anywhere else,
and there may well have not been enough time to make all the
arrangements.
As anticipated, the ECMO equipment relieved the stress on the
patients lungs, allowing them to heal while also arresting the HAP.
After three days, she had progressed enough to be taken off ECMO
and to resume treatment for her burn injuries.
Two months later, she was released. Today, her life is much as it was
before her accident.
That we were able to save a patients life is, of course, the most
satisfying outcome, Dr. Jeng says, but we also gained some new
insights into the use of ECMO. We demonstrated that someone
whod be considered a non-candidate anywhere else could benefit
from it, and that ECMO is something that needs to be taken seriously
for every case.
Equally important, Dr. Jeng adds, is the collaboration and
coordination of many Hospital Center physicians and departments to
bring together this patient and her life-saving treatment, a critical
element under such demanding, time-sensitive conditions.
A perfect storm of conditions were necessary to make this work,
and they all happened, he says. Looking back, it was really tearful to
see it all come together. n
JimParsons
O U T C O ME
Were Listening to You,
Acting on Your Concerns
by Janis M. Orlowski, MD, MACP
James C. Jeng, MD
The MedStar Brand: Redening Who We Are
Weve been a systemMedStar Healthfor more than 12 years. Our desire to
serve our communities and the ever-changing healthcare landscape led us to
begin a branding review to see who we are now and to explore the opportunity
to be the trusted healthcare leader in the Maryland and Washington, D.C., region.
We learned that to best position MedStar for the future, we would need
to focus onand celebrateour own unique strengths:
We creare knowlece rhrouh research, increase knowlece rhrouh
academics and apply knowledge in our clinical settings
We have rhe srrenrh, repurarion anc commirmenr ro provice
compassionate care
We have superior poinrs ol access lor parienrsmore rhan 100
community locations
These three unique strengthsknowledge, compassionate care and access
are the foundation for MedStar Healths rebranding, which has led to the new
tagline we will use across the system:
New Positioning. New Tagline.
begin a branding r
m m o c r u o e v r e s
eve been a systemMedStar Healthfor mor W
dS e The M
e now who we ar eview to see begin a branding r
g n a h c - r e v e e h t d n a s e i t i n u m
eve been a systemMedStar Healthfor mor
ening d e R and: r tar B dS
e the opportunity and to explor e now e now
e l e p a c s d n a l e r a c h t l a e h g n i
e than 12 years. Our desir eve been a systemMedStar Healthfor mor
r A e WWe ho WWho ening
e the opportunity
o t s u d e
e to e than 12 years. Our desir
e r
N
tagline we will use acr
e the foundation for MedStar Health ar
These thr
N ning. io osit w P e
oss the system: tagline we will use acr
e the foundation for MedStar Health
engthsknowledge, compassionate car ee unique str These thr
line. ag w T w Tag e N
oss the system:
ebranding, which has led to the new s r e the foundation for MedStar Health e the foundation for MedStar Healths r
engthsknowledge, compassionate car
ebranding, which has led to the new
e and access engthsknowledge, compassionate car
compassionate car
rhe have e W
academics and apply knowledge in our clinical settings
knowlece eare cr e W
to focus onand celebrateour own unique str
e learned that to best position MedStar for the futur W
d e t s u r t e h t e b o t
begin a branding r
e compassionate car
commirmenr anc epurarion r enrh, srr rhe
academics and apply knowledge in our clinical settings
ch, esear r ouh rhr knowlece
to focus onand celebrateour own unique str
e learned that to best position MedStar for the futur
a M e h t n i r e d a e l e r a c h t l a e h d
e now who we ar eview to see begin a branding r
ovice pr ro commirmenr
academics and apply knowledge in our clinical settings
ouh rhr knowlece ease incr ch,
engths: to focus onand celebrateour own unique str
e, we would need e learned that to best position MedStar for the futur
. C . D , n o t g n i h s a W d n a d n a l y r
e the opportunity and to explor e now e now and to explor
ouh
e, we would need
. n o i g e r ,
e the opportunity
tagline we will use acr
oss the system: tagline we will use acr
oss the system:
y t i n u m m o c
u s e v a h e W
compassionate car
locations
p r o l s s e c c a l o s r n i o p r o i r e p
0 0 1 n a h r e r o m s r n e i r a p
This is the logical next step in MedStars evolution as
the leading provider of healthcare services across
Maryland and the Washington, D.C., region, Samet
notes. This will be good for our organization, and
good for the communities we serve. n
5
MedStar Health Rebranding:
Coming Together Under One Name
4
C O V E R S T O R Y
The MedStar Brand:
Redening Who We Are
MedStar Health
Home to 27,000 medical professionals
6,000 physicians
More than 100 community locations
And 9 amazing hospitals
All focused on you.
medstarhealth.org
e Medical Center
MedStar Georgetown University Hospital
MedStar Good Samaritan Hospital
MedStar Harbor Hospital
MedStar Montgomery Medical Center
MedStar National Rehabilitation Network
MedStar St. Marys Hospital
MedStar St. Mary
MedStar Union Memorial Hospital
MedStar Washington Hospital Center
MedStar Family Choice
MedStar Health Centers
MedStar Visiting Nurse Association
MedStar Institute for Innovation
MedStar Health Research Institute
When youre sick or injured, you deserve the very best treatment every time. Thats why every
one of MedStar Healths locations is backed by the immense resources of tens of thousands of
medical professionals, 9 amazing hospitals and more than 100 community locations. Its our way
of ensuring you dont just get the best treatment a hospital can provide but the best treatment
our entire system can provide.
Why one health system flies
way above expectations.
medstarhealth.org
MedStar Franklin Square Medical Center
MedStar Georgetown University Hospital
MedStar Good Samaritan Hospital
MedStar Harbor Hospital
MedStar Montgomery Medical Center
MedStar National Rehabilitation Network
MedStar St. Marys Hospital
MedStar Union Memorial Hospital
MedStar Washington Hospital Center
MedStar Family Choice
MedStar Health Centers
MedStar Visiting Nurse Association
MedStar Institute for Innovation
MedStar Health Research Institute
5 4 JAN/FEB 2012 | PHYSICIAN | MEDSTAR WASHINGTON HOSPITAL CENTER MEDSTAR WASHINGTON HOSPITAL CENTER | PHYSICIAN | JAN/FEB 2012
We are now MedStar Washington Hospital Center.
I am pleased to announce the new branding of the entire MedStar
system, says Kenneth A. Samet, president and CEO, MedStar
Health. Our individual facilities have built strong historic identities.
Now each will share in the strength of being part of something
significantly bigger.
This unified name, MedStar
Health, will help us to achieve
our vision of being the trusted
leader for health care in the
region, Samet explains. In his
book, Good to Great, author Jim
Collins explains that for an
organization to achieve
greatness, it must embrace its
vision, be passionate about
continuous improvement and
create a more satisfying work
environment, where everyone
feels connected to the
organizations success. I believe
our new branding effort will not
only help to take us from good
to great, it will prove to be exactly what we need to build the
extraordinary MedStar Health of the future.
The newly unified MedStar Health will focus on our comprehensive
services, expertise, innovation, and technologywhile continuing to
promote the individual strengths of each MedStar site. It allows us to
give patients easier, more convenient access to all our facilities,
physicians and technologythe 27,000 associates, 6,000 physicians,
nine hospitals, and more than 100 community locations.
By joining all the MedStar Health facilities together more formally
under the MedStar name, we will be able to take better advantage of
our combined strength, which will raise the level of care throughout
each individual hospital and community location.
Our new branding and naming strategy shifts MedStar to an
all-for-one focus, which promotes our hospitals and sites
regionally, while raising the performance level of all. In addition,
we will have a new, unified tagline for each MedStar Health hospital
and site: Knowledge and Compassion, Focused on You.
The new tagline celebrates the three unique strengths of MedStar
Health:
n Knowledgecreating knowledge through research, increasing
knowledge through academics and applying knowledge in clinical
settings
n Compassionate carea consistently safe, high quality patient
experience provided in a patient first environment
n Superior accesswith more than 100 community locations
across the region
The rebranding effort includes an advertising campaign to educate
the community about the new MedStar Health. There are two
television ads, print ads and online advertising promoting
MedStar Health and the network of care available to patients.
The television ads and an educational video can be seen at
www.medstarhealth.org/brand.
The co-branding of the nine hospitals means each will start with the
MedStar name. Two of the hospitals are being updated, MedStar
Montgomery Medical Center and MedStar Franklin Square Medical
Center. MedStar National Rehabilitation Hospitals name remains
the same, but the extensive system of outpatient providers and
services are now MedStar National Rehabilitation Network.
In addition to redefining MedStar Health as an organization, all
physicians, nurses, and associates are recommitting to putting
patients first, and advancing the health of patients and their families.
Ken Samet
7
JAN/FEB 2012 | PHYSICIAN | MEDSTAR WASHINGTON HOSPITAL CENTER
7
Envision researchers as wild-eyed, bent
over the microscope, looking for a better way to treat disease.
You might need to re-shape your image.
While laboratory research is still vital to advancing health care, the
model for research is becoming more clinical outcomes-driven,
and MedStar Washington Hospital Center hopes to benefit from
that shift in focus.
Neil Weissman, MD, president,
MedStar Health Research Institute
(MHRI), says, Academic
medicine has traditionally been
only at a university hospital.
University hospitals are like three-
legged stools: one for teaching, one
for research and one for patient
care. You need all three legs of
equal strength, or it doesnt
stand.
The shift in the research model is
occurring because there is greater
demand to improve the efficiency
of health care, by exploring utility
of new diagnostics, new therapies
or new methods to deliver health care.
The Hospital Center is an independent academic medical
center, says Dr. Weissman, with a large base of clinical care
closely connected to our community. On that foundation of care,
were building research and education. Think of a tricycle. The
big wheel is the clinical machine. The small wheels are research
and education. Take any one wheel away, and the tricycle does not
move. The primary goal of the hospital is taking care of patients,
but excellence is going to come from having a milieu of research
and education. Furthermore, the large base of clinical care allows
us to create knowledge through research that remains focused on
our patients.
He explains, With even greater pressures on health care reform
looming, research needs to focus on efficiency and effectiveness in
patient outcomes. Dont just create another type of anti-platelet to
thin the blood. Instead, lets determine why so many people who
should be taking aspirin, which costs a penny a day, arent taking
it. Thats a better use of our money than spending a billion dollars
creating another derivative of aspirin. Its essentially research on
delivery of care. Its not quite as sexy, but it can make a great
difference to so many people.
Can you do this type of research at isolated, high-end hospitals?
Dr. Weissman continues. No. They are not representative of the
rest of U.S. health care. The Hospital Center and MedStar Health
are where academics and the real world come together. If it works
here, it can work anywhere.
The following are just a few examples of how the Hospital Center
is advancing health through research.
Burn Research
Burn Surgery is currently a
robust area of research at the
Hospital Center. Marion
Jordan, MD, FACS, director,
The Burn Center, said the
stars aligned in the last
couple of years, and we
suddenly had a renewed
energy, with two clinical
fellows and an additional
fellow who was specifically
interested in starting a
research program.
Concurrently, the D.C.
Firefighters Burn Foundation
offered to help us, by
renovating the physical space
in the research building.
As a result, several studies and projects are now underway, with
Jeffrey Shupp, MD, taking the lead. Dr. Jordan says, Dr. Shupp
has an extensive background in research and has developed many
contacts from his previous work. Hes like the Pied Piper in terms
of meeting and attracting collaborators, volunteers and students
from a variety of institutions to help us. The program at this point
is on firm footing with grants to support key personnel, such as
Lauren Moffatt, PhD (senior scientist) and Kate Flanagan, BS
(clinical research coordinator). Currently, our research breadth is
vast; encompassing everything from molecular pathophysiology,
to clinical trials involving improving pain after injury.
Research is Not Your Fathers Oldsmobile
6 MEDSTAR WASHINGTON HOSPITAL CENTER | PHYSICIAN | JAN/FEB 2012 6
F E AT U R E
Cardiovascular Research
Another area of research
strength is in cardiovascular
disease. Research in the
cardiovascular area is critical
to patient care, and for a large
center like ours, its also our
responsibility, says Stuart F.
Seides, MD, physician
executive director, MedStar
Heart Institute. We are a
regional and national referral
center with a high
concentration of physicians
and physician researchers
with expertise in a large
number of diagnostic and
therapeutic modalities. As a
result, we really have a responsibility to gather information,
process it and come up with data that ultimately allows physicians
here, and in the larger medical community, to make the best
decisions they can for individual patients.
Dr. Seides continues, The work of Federico Asch, MD, is a good
example of our research efforts. Dr. Asch helps manage the
Cardiac Imaging Core Lab, where we look at outcomes of new
procedures across the globe to categorize their benefits in a
consistent and believable way. Dr. Asch is working on a national
registry that allows us to pool a significant number of patients for
cardiac diseases that are uncommon but not rare. Where
individual centers would see only a modest number of patients
during a given period of time, the larger aggregation of consistent
data enables us to draw conclusions that are statistically relevant.
Instead of having five or six patients, we have more than 3,000
patients. From that data, we can draw conclusions both
diagnostically and therapeutically about the best way to diagnose,
follow and treat those individuals.
Neil Weissman, MD
Marion Jordan, MD
Stuart Seides, MD
Academic medicine has traditionally been only at a university hospital.
University hospitals are like three-legged stools: one for teaching, one for research and
one for patient care. You need all three legs of equal strength, or it doesnt stand.
Jeffrey Shupp, MD
Jeffrey Shupp, MD, admits his interest in research was born when he got a job washing dishes in a
research lab, as an undergraduate at University of Maryland. He has since transitioned from lab
prep work, and is now actively engaged in many MHRI research projects, clinical trials and
collaborations.
A focus of Dr. Shupps research is the study of the pathobiology of cutaneous wounds, which
envelops burn wound healing, chronic wound healing, and hyperproliferative scarring. The
research group has received funding from the NIH to study the effects of pressure therapy on the
healing of scars. This project is in collaboration with researchers at The Catholic University of
America, where Dr. Shupp is an assistant professor of Biomedical Engineering.
The lab also focuses on surgical infectious complications and the hosts response to bacterial virulence factors. One study
underway examines the effectiveness of different types of antibiotics on burn wound infections. This study not only looks at the
benefits of the drugs in clearing infection and in wound healing, but also examines the systemic impacts of the bacteria on the
host. Dr. Shupp says, This is a true bench-to-bedside project, where we are modeling pathology in the laboratory and
concurrently designing and implementing observational clinical trials in our patients who are injured by burns.
A new area of research we are excited to work on is the study of occult coagulopathy in burn patients, he says. Were not really
sure what happens in the microvasculature of burn patients, and perturbations of the clotting cascade may influence burn depth
progression. The prospective studies start as soon as the patients enter MedSTAR Trauma. Well acquire blood samples from them
at hour zero and then hourly for the first 48 hours, and then a few days out after that, and we just measure different coagulopathic
markers in the blood.
This study is funded by the Department of the Army, and the Hospital Center is the only site to be enrolling burn patients.
Through collaboration, he adds, our research program has been able to build a foundation for success. Conducting, presenting,
and publishing research is an ultimate way to demonstrate to the community and our patients that we are working to be a leading
health system.
9
JAN/FEB 2012 | PHYSICIAN | MEDSTAR WASHINGTON HOSPITAL CENTER
9
Advancing Health Through Research
Last October, about 25 MedStar
Health physicians, PhDs, nurses
and administrators gathered on
Marylands Eastern Shore for a
two-day retreat. They
strategized ways to advance the
research contribution MedStar
makes in health and innovation,
and discussed system-wide
collaboration. They examined
MedStar Healths ability to
engage the community in the
care process, and become
positioned as an academic
medical system that provides care and creates knowledge.
Allen Taylor, MD, chief, Cardiology Division at MedStar
Georgetown University Hospital, moderated the retreat. We
want cooperation across our geographically dispersed hospitals
acting as a system, he says, and research is a really important
paradigm for that system. Its not just discoveries, but using
knowledge development to help the organization advance.
Dr. Taylor continues, Weve got a dizzying array of projects and
are receiving funding from federal agencies as well as
collaborations with universities. Traditionally, our research is
working in a lab, but now its also about analyzing information so
the organization can understand quality and outcomes. We can
learn what works best. n
Norma Babington
8 MEDSTAR WASHINGTON HOSPITAL CENTER | PHYSICIAN | JAN/FEB 2012 8
F E AT U R E C O N T I N U E D
State of the Heart
A Year of Progress for
MedStar Heart Institute
by Stuart F. Seides, MD, physician executive director, MedStar Heart Institute
Its beena little more than a year since the inception of
MedStar Heart Institutea pioneering model of organizational
management and enhanced cardiovascular care. We set an ambitious
agenda for the Institute at the start, and we have accomplished a great
deal. These successes have bolstered our vision for the Institute as an
integrated system of cardiovascular care for the regionand an
incubator for the continuing development of unique approaches to
cardiac treatment and care delivery.
Creating strong independent leadership and governance has been a
key element in the Institutes development as a hospital within a
hospital. Weve put management in the hands of the
multidisciplinary team of physicians and nurses who deliver
cardiovascular carea true service-line structure that allows us to
sustain streamlined and efficient operations, while promoting
superiority in patient services across the care continuum.
In recent months, we added three skilled leaders to the Institute team.
Ann Marie Madden, RN, MS, CCRN, NEA-BC, is assistant vice
president for Nursing and Brad Kappalman is our chief
administrative officer. Allen Taylor, MD, FACC, FAHA, has assumed a
new role in the Institute as chief, Cardiology Division for MedStar
Georgetown University Hospital.
On another front, a newly-organized Credentialed Advanced
Practice Clinician Leadership Committee serves as a forum of ideas
and information exchange for the Institutes nurse practitioner
practice, which has long-played a significant role in frontline cardiac
care delivery. A number of internal operational improvements have
been implemented. Two new cardiac catheterization labs (CCL) have
been added in support of our growing program, already the nations
busiest. Concurrently, we introduced a number of new processes in
the CCL to improve efficiency and throughput. Finally, in the next
few months we will complete the renovation and upgrade of our
existing Electrophysiology Labs (EPL),
We continue to identify ways for managing costs more effectively.
For example, supply chain savings have been enhanced significantly
through creating an expectation of accountability for individuals at
all process levels. We also intend to introduce a new data
management system for case management of CCL and EPL patients.
The system will allow enhanced data collection and provide critical
information necessary to conduct clinical research as well as help to
reduce duplication of effort, streamlining workflow. We see this
system as a precursor to a system-wide integrated electronic medical
record that will cross clinical disciplines and patient care settings
throughout the MedStar Health network.
More coordinated approaches to cardiac care delivery among
MedStar Health sister hospitals are being explored. Already
well-established is a systemic approach to managing advanced heart
failure across Baltimore-Washington regions, through standardizing
clinical protocols and physician order sets, and generally creating a
funnel whereby patients have multiple access points to the full array
of diagnostic and therapeutic options available for the treatment of
advanced heart failure.
A Womens Heart Program will soon be located at the MedStar
Health Center in Chevy Chase, Md., staffed by a cadre of MedStar
Heart cardiologists with special interest, expertise and experience in
the prevention, diagnosis and treatment of heart disease in women.
This will be the first of a number of cardiology specialty programs we
hope to co-locate in MedStar Health ambulatory care centers in the
Washington, D.C. region.
External networking has garnered us the first of a number of planned
affiliations with hospitals throughout the region. MedStar Heart
Institute and Reston Hospital Center entered into a collaborative
agreement to broaden the scope of advanced services and specialized
expertise available to heart patients in Northern Virginia. Specifically,
MedStar Heart will offer patients access to highly-developed
advanced heart failure care, including LVAD implantation as well as
provide surgical back up and general access to our tertiary-level
cardiovascular services through MedSTAR Transport Services. We
also are aggressively seeking partnerships with independent
cardiology practices, through collaborations fashioned to broaden
and strengthen the scope of MedStar Heart services.
For more than 50 years, cardiovascular services at the Hospital
Center have maintained a position of consistent preeminence in the
field through an international reputation for innovation and
excellence. It is our mission to carry on this program legacy through
MedStar Heart Institute. We believe that we can further enhance our
position through continuing operational improvement and financial
success, which importantly, will enable us, in todays challenging
health care environment, to offer the most sophisticated and
compassionate heart care to the people of our region. And that, truly,
is our raison dtre. n
Stuart F. Seides, MD, can be reached at stuart.f.seides@medstar.net.
U P D AT E
Federico Asch, MD
Federico Asch, MD, came to the Hospital Center from his native Argentina to pursue a fellowship in
echocardiography. As part of his fellowship, he worked in the Cardiovascular Imaging Core Lab with
Dr. Neil Weissman. Dr Asch says, I started to get more engaged in research activities at different levels,
and thats when I decided rather than return to my home in Argentina, I wanted to stay here.
In the Core Lab, where he is the associate director, he and five other physicians and 10 technologists
and fellows are working on about 30 active clinical studies. By imaging the heart and vessels, most of
their research addresses the safety and efficacy of novel cardiovascular therapies.
For example, he explains, a company develops a new type of artificial heart valve and wants to
know if it works well and is safe. We design an imaging protocol that best fits their needs, and train
sites all over the world in obtaining the images in a standardized fashion. The enrolling centers acquire the images from their patients
and send them to us for a central, standardized, independent analysis. The information we get from the image analysis is then used to
determine further product development, publications and, ultimately, FDA approval.
In addition, Dr. Asch performs investigator-initiated activities supported by NIH/NHLBI grants. He is currently PI for a national study
of patients with genetically related thoracic aortic aneurysms called Genetically Triggered Thoracic Aortic Aneurysms and
Cardiovascular Conditions (GenTAC). This project involves more than 4,000 patients with dilated aortas related to conditions such as
Marfan syndrome, bicuspid aortic valve, Turners syndrome, Ehlers-Danlos, familial aneurysm and others.
Were trying to get a better understanding on the characteristics and outcomes of these patients, he says. All patient images
(echocardiograms, CT and MRI) from the eight national leading centers are being sent to the Core Lab for analysis. The imaging
database we are generating will be merged with genetic, clinical, phenotypic and biomarkers databases, providing an unprecedented,
unique opportunity to understand a population that carries an enormous risk of aortic dissection and death.
Dr. Asch says, This study appealed to me, because our knowledge about these diseases is limited. Theyre hard to study, because its
difficult to put together a large number of patients without a national consortium. I am proud to be part of this nationally recognized
team and adding our expertise in cardiovascular imaging.
He adds, To me, from a career standpoint, it is a unique and exciting moment. Being an important piece of this project allows me to
work side by side with national leaders, a group of elite investigators in the field who are working in all aspects of these diseases, from
the bench labs to the clinic and the operating rooms. As a young investigator, this opportunity is precious, and its value limitless.
Stuart F. Seides, MD, physician executive director, MedStar Heart Institute, agrees. The Core Lab gives our young researchers and
fellows an opportunity to learn about the research process and get them enthused about cardiovascular research and their own
careersand theres a sense of responsibility. We, as one of the largest cardiac centers in the country, have a responsibility to move the
knowledge and progress forward, leveraging the resources we have by virtue of both our large patient volume, and the expertise of our
physicians and physician researchers.
Allen Taylor, MD
11
JAN/FEB 2012 | PHYSICIAN | MEDSTAR WASHINGTON HOSPITAL CENTER
11 10 MEDSTAR WASHINGTON HOSPITAL CENTER | PHYSICIAN | JAN/FEB 2012 10
Informed
Consent
Update
by Nneka Mokwunye, PhD, director, The Center for Ethics
Customizedinformed consent forms for each medical
and surgical procedure will make the consent process more specific
for physicians, and more meaningful for patients. The hospital-
wide effort is in response to the Centers for Medicare and Medicaid
Services (CMS) and The Joint Commission requirements.
Physicians every day engage in discussions with their patients,
explaining diseases and disorders and outlining treatment options.
But informed consent takes the discussion to the next level. When
a patient agrees to a procedure, the informed consent process calls
for complete disclosure of the risks, benefits and alternatives for
that procedure. It also requires physicians to determine patients
ability to fully comprehend what they are about to undergo.
Soon that process will work better for both physicians and
patients. Each department and section in the hospital is developing
customized consent forms for procedures that are most frequently
performed. The new forms will have a preprinted summary of the
procedure, plus the potential risks, benefits and alternatives for the
procedure. The forms also address the reason for the procedure,
and the likely outcome of not having the procedure. These forms
will replace the standard, generic informed consent forms. The
Center for Ethics has templates that can be adapted to each
procedure.
A key component of these individualized forms is readability.
Physicians need to make sure that patients and family members
really understand what they are telling them. Often patients will
nod as if they understand, but not all do, and they are afraid to
ask questions.
The intent is for each consent form to be written at an eighth-
grade level, and avoid med-speak. The staff of the Center for
Ethics reviews each template, and simplifies wording when
necessary. All completed informed consent forms will be available
on the Clinical Documents Repository for easy access.
Consent is a process. Its not just documents. Its a conversation
that may take multiple visits to complete. Its important that
patients understand the risks, benefits and alternatives for the
procedure. They need to be able to ask questions and get answers
that they can understand. n
For more information, call Nneka Mokwunye, PhD, at 202-877-6211.
Personalized care is the new horizon in oncology,
with exquisitely detailed genetic information that revolutionizes
risk-assessment, screening and treatment. At the same time, this
personalized approach represents a daunting but doable challenge
to basic science researchers.
Personalized medicine centers on the decoding of oncogenes and of
the proteins they code. Simply put, oncogenes have the potential to
drive the malignant transformation of normal cells by triggering
specific protein-signaling cascades. By decoding these genomes, the
way is paved to truly personalize medicine through genetic testing,
targeted cancer screening and prevention, and targeted therapy that
produces better results and fewer side effects.
In the last decade or more, professional meetings have included
sessions on cancer genetics, says Lawrence Lessin, MD, an
oncologist, director of Continuing Medical Education and former
director of Washington Cancer Institute. The effort to identify
cancer-causing genes and their protein products will have a major
impact across the medical field, both for public health and for
disease management.
When President Nixon declared The War on Cancer in 1971, the
scientific community believed that a cancer cure was within reach.
But the target has changed dramatically in the intervening years,
with clinicians and researchers now focusing on cancer control.
The effort to identify the mechanics of cancer signals a shift from
a clinical focus to a basic science focus. This has tremendous
importance to cancer care, says Sandra M. Swain, MD, an
oncologist and medical director of Washington Cancer Institute.
It will have an impact on other disease entities as well.
Scientists completed the decoding of the Human Genome in 2007,
presenting a baseline look at some 20,000 genes in the human body.
It is not farfetched to think that each person may have his or her
own decoded genome readily available in the not-too-distant future.
The logical next step is to develop a map of the Cancer Genome,
which is now underway. This project seeks to identify genes that are
critical in the development of human cancer. Other genes of interest
are tumor suppressor genes, which turn off the malignant process,
but fail to do so when mutated. As genes are identified, they become
part of the Cancer Genome Atlas, a repository of shared data being
compiled by the National Institutes of Health (NIH).
This is a much more complex task than mapping the human
genome. There may be 80 to 90 mutations in breast tumors alone,
Dr. Swain explains. We have to identify which are the most
significant mutations. Today, breast tumors routinely are
genotyped before treatment begins, so treatment will be targeted to
individual cancers.
Farther down the research road is the proteome, comprising the
proteins involved in specific signaling pathways. Proteomics will
determine which proteins are responsible for switching on
malignant growth, stimulating the development of a blood supply,
ordering the metastatic process, and making the malignant cells
immortal. This is a level of molecular information even more
specific, because protein signaling pathways that drive mutation can
be altered in a number of different ways, even if the genome is the
same. A study showed that an average of 13 protein pathways are
disrupted in a cancer cell.
As the research becomes more specific, we will learn a lot. This is
data mining, really, Dr. Swain notes. The goal is to find the key to
what is going on in malignant cells, so we can target specific
mutations or proteins in cancer, and then individualize therapy.
The first chromosomal abnormality to be linked to specific cancers
was the Philadelphia Chromosome, a 9-22 translocation first
identified in 1960, which was linked to chronic myelogenous
leukemia (CML). With this knowledge, imatinib (Gleevec) was
developed to target the BCR-ABL fusion gene and switch it off.
Imatinib now is used to treat gastrointestinal stromal tumors (GIST)
as well, targeting the c-kit mutation.
Most of the recent successes in targeted therapy have been
antibodies that target specific proteins, and either disrupt the
malignant process or deliver chemotherapy to the malignant cell in a
precise way. Protein kinase inhibitors are enzyme inhibitors that
block the action of kinases, proteins essential to transmit activation
messages in the cells, and also switch off the malignancy.
Already a dozen or more targeted drugs have completed clinical
trials and are now treating melanoma, breast cancer, kidney cancer,
GIST and some types of leukemia (including CML) and lymphoma.
These new targeted therapies are highly specific molecules, many in
pill form. They target malignant cells precisely, with less damage to
healthy tissues and fewer side effects.
This is part of the dream for everyone working with cancer,
says Raquel Nunes, MD, an oncology fellow at the Hospital
Center. Weve recognized for a long time that we dont know
how to treat cancer in an intelligent way. Ultimately, its a genetic
disease. By deciphering the code and its downstream products,
we will better understand the disease and better treat it.
Most targeted therapies are used in conjunction with
chemotherapy to control cancers, significantly extending
survival. But in some caseslike melanoma, hepatocellular
carcinoma, GIST and kidney cancervirtually no effective
treatment existed until targeted therapy was introduced.
Although cures are still rare, the advent of these treatments
proves the principle behind the research and is only the
beginning of a totally new era in cancer treatment.
This basic science thrust to understand the underpinnings of
malignancy follows decades spent developing chemotherapy
protocols. Treatment has been empirical, Dr. Lessin says. In
the next decade, more cancers will be treated based on their
genomic and proteonomic profile rather than histopathology,
and more will be characterized by different genetic subtypes,
leading to individualized treatments.
While Washington Cancer Institute does not have its own basic
science research lab, its researchers work closely with outside labs
and researchers and participate in many clinical trials with
MedStar Georgetown University Hospital and NIH. The Cancer
Institute is conducting a study on genomic profiling in breast
cancer (the MammaPrint study), a genomics study that stratifies
women into low- or high-risk of breast cancer recurrence, and
characterizes the tumor at the molecular level. The Cancer
Institute also is collaborating with George Mason University in a
proteomics study of pancreatic cancer, using a novel method to
look at very low levels of proteins in the blood and establish a
protein map in pancreatic cancer, a highly fatal disease for which
new treatments are needed.
In the next quarter century, Dr. Lessin predicts that cancer
treatments will become more and more targeted to the genetic
profiles of individual tumors. Cancer risk assessments will be
more finely tuned, and cancer screening will be risk-stratified.
And when cancer does occur, it will be treated more as a chronic
disease, with less toxicity and more effective management.
Will there ever be an end to cancer? When DNA is replicated,
intrinsic errors occur, Dr. Lessin says. Mutations can be caused
by both environmental and intrinsic factors, which can led to
malignant transformation.
You never know when the next major breakthrough will
happen, Dr. Swain concludes. n
Catherine Avery
The New Horizon for Cancer Care
N E WS
Lawrence Lessin, MD Sandra M. Swain, MD Raquel Nunes, MD
N E WS
13
JAN/FEB 2012 | PHYSICIAN | MEDSTAR WASHINGTON HOSPITAL CENTER
13
We are workingto help improve your patients care,
and ease your communications with others by changing three major
IS clinician applications at MedStar Washington Hospital Center.
The physician informatics group will keep you up-to-date on
ongoing changes via DocsLink, which is emailed to all of you every
Friday morning at 7.
Microsoft Office/Outlook Conversion
Following the Microsoft Office/Outlook 2007 conversion, all
MedStar computer users (except at MedStar St. Marys Hospital
and MedStar Montgomery Medical Center) are on the same email
platform, and use the same version of Microsoft Office. Although
email is no longer sent to Lotus Notes, the icon remains on desktops,
and you can access all Lotus Notes databases.
There are significant differences with Office 2007; for example, the
toolbar in Word has a different look. Training opportunities for
Office and Outlook include lectures, hands-on demonstrations and
online training on SiTEL. These are being scheduled via SiTEL
(http://www.whc.sitelms.org). The IS Migration Team provides
newsletters, email notifications and updates via the Microsoft
Office/Outlook 2007 Migration website in StarPort.
Azyxxi to Amalga Conversion
Amalga replaces Azyxxi as our system for viewing and analyzing
patient-centric clinical data. Amalga has a similar, look, feel and
functionality as Azyxxi, but allows for electronic viewing of both
inpatient and outpatient data from multiple MedStar hospitals.
The data includes:
nAria - Outpatient Oncology Electronic Health Record
(EHR) documents
nPeribirth - Obstetrics Inpatient EHR documents
nCentricity - Outpatient EHR documents limited clinics
nInpatient unit lists
nLab results
nImages
nRadiology reports
nInpatient medication lists
nOperative reports
nDischarge summary dictations
Inpatient medication reconciliation and discharge instructions are
also available in Amalga.
One of the biggest Amalga benefits is the access to patient data from
other MedStar hospitals, including labs and radiology reports, which
are displayed alongside Hospital Center data. You can access patient
records from other MedStar hospitals even if the patient has never
been to the Hospital Center.
Amalga also uses the same Network User ID and password that you
use for logging into the MedStar network, MedConnect and
Outlook. For security reasons, shared accounts are not supported in
Amalga.
Please start using Amalga as it is rolled out to your department.
Once the Amalga rollout is complete, Azyxxi will be phased out.
MedConnect
We continue to move toward a complete inpatient electronic health
record: MedConnect. It allows for patient data to be shared across
MedStar hospitals, except for St. Marys and Montgomery Medical
Center, which have separate EHRs.
To prepare for computerized provider order entry (CPOE), the
MedConnect EHR underwent a significant expansion in January.
We are asking for physicians to become familiar with the
MedConnect system before CPOE is implemented in Jan. 2013.
The EHR Expansion, or Phase Ib, included adding the following
interfaced patient data to MedConnect:
nEKG
nGI Lab
nCardiac Cath
nEchocardiology results
Developing and Improving
IS Clinician Applications
by Peter C. Hill, MD, Chief Medical Information Officer
12 MEDSTAR WASHINGTON HOSPITAL CENTER | PHYSICIAN | JAN/FEB 2012 12
N E WS
nDictations and radiology reports
nSummary documents from Aria and Peribirth.
Radiology images are currently unavailable, but there are plans to
add this feature. Outpatient Centricity data is also unavailable at
this time.
With the EHR Expansion, you can see:
nPatient Lists
nPatient Summary
nResults Review
nMicro Viewer
nPhysician Work List
nRemote access via the Clinician Portal
Patient Summary allows you to view detailed information for a
selected patient from a single summary page. You can drill down
the patient chart to review specific information, including recent
vital signs, intake and output, by simply double-clicking on the
patients name.
Self-training materials and group demos are currently available for
Hospital Center providers. Optional classroom training will occur
in April, with a supported go-live scheduled for May. The MedStar
Training team will be asking for clinician super-users to assist with
education and training during this roll-out period, and volunteers
are appreciated.
Next Steps in Building MedConnect
Phase II, also known as MedConnect II, is expected be completed in
early 2013. It includes:
nComputerized Provider Order Entry (CPOE)
nInterdisciplinary Plans of Care (IPOC)
nMessage Center
nDepart Process
nEmergency Department module
nPerioperative module
nUpgrade to nursing documentation
When this phase is completed, physicians, nurses, pharmacists and
other caregivers can view patient data, consider evidence, enter orders,
document their actions and share information in a single patient
record. Physicians will continue to document on paper.
As a prequel to CPOE, evidence based order sets are being created by
interdisciplinary teams from each of MedStars hospitals with support
from Zynx Health, a nationally recognized clinical content provider.
Order sets are being developed in waves until all orders are completed.
MedStar Union Memorial Hospital will be the first in the system to
use CPOE this summer. The Hospital Center CPOE go-live date is
scheduled for January 2013. Mandatory training for all providers is
expected to start six weeks before the go-live.
In Phase III, providers will move closer to paperless charting by
moving their documentation to MedConnect. Critical Care and
Anesthesia modules will also be added. This phase is tentatively
scheduled for 2014.
Thank you for your support as we work to improve the IS structure
for you and your patients. Please contact me if you have any
questions. n
Peter C. Hill, MD, is chief medical information officer. He can be
reached at peter.c.hill@medstar.net.
For the latest information on the MedConnect II Electronic Health
Record expansion, please visit the Connect II website in StarPort, or use
this link:
http://starport4.medstar.net/corp/is/medconnect/Pages/default.aspx.
For additional questions, please contact the Physician Informatics
Coordinators: Claribel Sawyerr at claribel.l.sawyerr@medstar.net and
Rodger Mateeka at rodger.m.mateeka@medstar.net.
For questions about the Office / Outlook 2007 Conversion, please
contact Melody Kokoszka, Medstar Health, at
melody.a.kokoszka@medstar.net, or 202-877-9095.
For questions about the Azyxxi to Amalga Conversion, please contact
David Hall, Amalga Roll-Out manager, at david.j.hall@medstar.net,
or 703-298-5921.
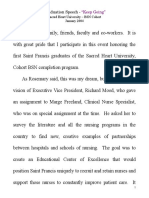
CuLlook / Cmce 2007
Mlgrauon
12/06/11 -02/02/12
Amalga
8oll CuL
12/07/12 - 02/03/12
MedConnecL MWPC
Work llow Locallzauon
01/09/12 - 02/ 06/12
MedConnecL Lxpanslon - Cllnlcal 8esulLs / 8emoLe Access
01/12
auenL LlsL and 1eams
03/07/12
MC hase ll
CCL
Lu
erlC
MuMP 07/12
MWPC 01/13
Crder SeL uevelopmenL
CompleLe 03/2012
uecember
2011
!anuary lebruary March Aprll May !une !uly
2012
PosplLal CenLer Cllnlcal Appllcauons
8C!LC1S 1lML LlnL
MedConnecL
hase l
Pharmacy Lab
Resp Therapy
Documentation
RN
Documentation
Positive Patient Identification / Bar Coded Med Administation
Clinical Results
CPOE ED
Peri Op
Services
Messaging
Center
PPID
Blood
Remote Access
Phase I
Phase Ib
Critical
Care
Anesthesia
Physician
Documentation
Phase II
Phase III
Fully Electronic MR
Data Warehousing / Mining
2013
2012 expansion
Complete
Building MedConnect
Inpatient EHR
Patient Lists
15
JAN/FEB 2012 | PHYSICIAN | MEDSTAR WASHINGTON HOSPITAL CENTER
15 14 MEDSTAR WASHINGTON HOSPITAL CENTER | PHYSICIAN | JAN/FEB 2012 14
N E WS & N O T E S
David Jeong, MD Allergy
Richard Morrissey, MD Cardiovascular Disease
Farooq Sheikh, MD Cardiovascular Disease
Shantanu Agrawal, MD Emergency Medicine
Dorota Krawjewski, MD Endocrinology
Dia Copeland, MD Gastroenterology
Rabindra Paul, MD Hematology Oncology
Matthew Memoli, MD Infectious Disease
Aakash Desai, MD Internal Medicine
Amit Desai, MD Internal Medicine
Ruta Dubinskaite, MD Internal Medicine
Tara Eastin, DO Internal Medicine
Omid Fatemi, MD Internal Medicine
Sa-Yun Hong, MD Internal Medicine
Nabeel Iman, MD Internal Medicine
Ning Jiang, MD Internal Medicine
Osaguona Osa, MD Internal Medicine
Ashley McClure, MD Internal Medicine
Joseph McDonald, MD Internal Medicine
Vikramjit Mukherjee, MD Internal Medicine
Shailesh Sheth, MD Internal Medicine
R. Kendall Smith, MD Internal Medicine
Manan Trivedi, MD Internal Medicine
Uzma Vaince, MD Internal Medicine
Gebremedhin Yohannes, MD Internal Medicine
Dana Best, MD Neonatology/Pediatrics
Fannie Brown, MD Neonatology/Pediatrics
Niti Dham, MD Neonatology/Pediatrics
Joshua Kantor, MD Neonatology/Pediatrics
Katie Gettings, NP Nephrology
Saurabh Goel, MD Nephrology
Jeffrey Komisarof, MD Nephrology
Ella Popeliansky, MD Neurology
Akua Afriyie-Gray, MD ObGyn
Ashley Hothem, MD ObGyn
Karishma Patel, MD ObGyn
Matthew Reeves, MD ObGyn
Lina Amini, MD Ophthalmology
Christopher Thiagarajah, MD Ophthalmology
Jill Bailey, DDS Oral & Maxillofacial
Surgery/Orthodontics
Rebecca MacIsaac, NP Orthopaedic Surgery
Irim Ciolino, MD Physical & Rehab Medicine
Maira OToole, PA Radiology
Ruchika Gutt, MD Radiation Oncology
Jennifer Verbesey, MD Transplant Surgery
Eboni Woodard, MD Urology
Robyn Macsata, MD Vascular Surgery
James Salander, MD Vascular Surgery
WELCOME TO
NEW ATTENDINGS
K. Eric De Jonge, MD and the Medical House Call Program team were awarded the Richard and Hilda Rosenthal
Award #2 from the Rosenthal Family Foundation. The award was given by the American College of Physicians for the
outstanding work done by Dr. De Jonge and his team. The award is presented "to that individual or organization,
whose recent original approach in the delivery of health care or in the design of facilities for its delivery will increase
its clinical and/or economic effectiveness."
AWARD FOR
DR. DE JONGE & MHCP
Augusto Pichard, MD, director of the Cath Lab and one of
the principal investigators of the CorPath PRECISE clinical trial, led
a team of interventional cardiologists, nurses and surgical
technicians using the CorPath 200 robotic surgical system.
This robot-assisted coronary angioplasty was the first in the region.
The team successfully opened a blocked artery for a 58-year-old
patient who was hospitalized for fewer than 24 hours before
discharge. The clinical trial is a multi-center study, which will enroll
up to 200 patients at medical centers nationwide.
Kudos to the Cath Lab
Allen Taylor, MD,
is the new chief of
Cardiology at MedStar
Georgetown University
Hospital. Dr. Taylor
served for three years as
director, Advanced
Cardiology Imaging at
the Hospital Center,
following 20 years as
director, Cardiovascular
Research at Walter Reed
Army Medical Center.
He is board certified in
internal medicine and
cardiovascular disease by
the American Board of Internal Medicine, and is a fellow of the
American Heart Association and the American College of
Cardiology. Dr. Taylor has held leadership appointments on
multiple national cardiology organizations and is widely published
in national medical journals. He has also been cited in many major
media outlets as an authority in cardiovascular disease.
Leadership Post for Dr. Taylor
The Medical House Call Program team includes (seated) Carrie Carmon, Nancy Sassa, NP; Mary McDonald, MD; Sandy Mills, Jan Goldberg, NP;
Robyn Feely, NP and Namirah Jamshed, MD. Standing are Eric De Jonge, MD; Katherine Baker, Nadine Hailu, Michelle Sullivan, NP; Stephanie
Bruce, MD; Julie Beecher and George Taler, MD. The top row finds Maria Copeland, LaWanda Holeman, Ruth Shea, LGSW; Rachel Lipman,
LGSW and Monica Thomas, LICSW. Not pictured are Karen Johnson, MD, Jennifer Crawley, LICSW and Sari Greene, LICSW.
Four physicians were named hospital SuperStars by patients and others, between April and September. They are Philip Fidler, MD,
The Burn Center; Praful Ramineni, MD, General Surgery; George Sample, MD, Critical Care/Trauma Services and Abubakari Welle, MD,
Department of Medicine Hospitalist Service.
Congratulations to Physician SuperStars
Philip Fidler, MD Praful Ramineni, MD George Sample, MD Abubakari Welle, MD
16 MEDSTAR WASHINGTON HOSPITAL CENTER | PHYSICIAN | JAN/FEB 2012 16 17 JAN/FEB 2012 | PHYSICIAN | MEDSTAR WASHINGTON HOSPITAL CENTER 17
D E PA R T ME N T O F C O N T I N U I N G ME D I C A L E D U C AT I O N A N D Q U A L I T Y T R A I N I N G
Quality and Outcomes Management:
Providing Framework for
Good Outcomes, Zero Defects
Physicians are trainedto practice evidence based
medicine to heal the sick and injured, and to keep the healthy well.
When they refer or admit their patients to a hospital, they want that
hospital to use evidence-based approaches, too. Doctors rely on a
hospitals infrastructure to ensure that their patients are safe and well
cared-for.
At MedStar Washington Hospital Center, the Outcomes Management
team provides the framework, expertise, guidance and support to
ensure that the physician/hospital partnership produces optimal
clinical outcomes, satisfied patients and importantly, optimizes
reimbursement. The team also provides consultation to physician
practices owned by the hospital.
In todays highly regulated health care environment, the outcomes
management team serves as a clearinghouse for current standards,
requirements, regulations and best practices set forth by The Joint
Commission (TJC), the District of Columbia, and the Centers for
Medicare and Medicaid Services (CMS). The team works with
physicians, nurses and other stakeholders throughout the hospital to
build teams and develop and implement processes that improve
clinical outcomes and ensure regulatory compliance. They collect
performance data and report the Hospital Centers results as required.
The team also leads the hospitals Culture of Safety program.
One example of the work of
the Outcomes Management
team was the organization of
performance improvement
(PI) teams around the core
quality measures designated by
Medicare. The measures are
based on best practices in the
treatment of pneumonia,
heart failure, acute myocardial
infarction and certain surgical
procedures.
Sunil Madan, MD, medical
director of the hospitals
Department of Emergency
Medicine, leads the
pneumonia PI team. It
developed and implemented a
clinical pathway and physician
order sets based on best practices
in pneumonia care. These best practices included antibiotic selection
and timing, blood cultures, vaccine screening and discharge
education.
Evidence, as well as our experience after implementing the pathway,
demonstrates that by following these processes in the treatment of
pneumonia, patients get better care, leave the hospital faster, have
fewer readmissions, and experience lower mortality, Dr. Madan says.
The pneumonia PI team is helping optimize the care of pneumonia
patients throughout the hospital.
Pneumonia isnt the only area that experienced improved outcomes.
Last year, the Hospital Center received the 2011 Excellence Award for
quality improvement in Hospitals from the Delmarva Foundation, for
sustained and improved quality performance in all four clinical areas.
As Medicare continues its transition to a pay for performance
model, hospitals that use best practices and perform well on the core
measures benefit financially. Currently, the financial risk of providing
poor care lies solely with the hospital. However, it is anticipated that
eventually, Medicare will bundle hospital and provider payments,
based on both parties performance.
Once Medicare begins to
bundle payments to hospitals
and providers, we predict that
other payors will follow, just as
they have done in the past,
says Mary-Michael Brown,
DPN, RN, assistant vice
president for Quality and
Outcomes. Payors want to
pay for safe, quality care, and
define quality as following
evidence-based approaches,
best practices, and performing
well in the core measures. As
to the transparency of the
health care industry, she says,
The data we report to
government agencies,
including patient outcomes
and satisfaction, is now
available on the Internet.
Still, while changes in the health care landscape have created financial
challenges for physician practices and hospitals alike, all are still driven
by what is best for the patient. Providers want to do the right thing,
adds Brown. The Outcomes Management team is here to help. n
Lynn Cantwell
N E WS
Upcoming CME Conferences
REGULARLY SCHEDULED SERIESAMA PRA Category 1 Credit(s) UPCOMING CONTINUING
MEDICAL EDUCATION
CONFERENCES
FEBRUARY 25-27, 2012
Electrophysiology 2012:
Straight Talk From the
Experts
AdamStrickberger, MD
& George Klein, MD
Activity Directors
Lion Square Lodge
Vail, Colorado
FEBRUARY 26-28, 2012
Controversies in Medicine
2012
Paul J. Corso, MD &
Lawrence S. Lessin, MD
Activity Directors
Lion Square Lodge
Vail, Colorado
MARCH 3, 2012
Lung Cancer 2012:
The New Paradigm
Keith D. Mortman, MD
& Mark S. Soberman, MD
Activity Directors
Hotel Monaco
Washington, D.C.
MARCH 14, 2012
Childrens National
Medical Center Pediatric
Neurology Update 2012
Roger J. Packer, MD
Activity Directors
Childrens National
Medical Center
Washington, D.C.
MARCH 23-24, 2012
Advances in Breast
Cancer 2012
Pamela Randolph-Jackson, MD,
Minetta C. Liu, MD &
Chika N. Madu, MD
Activity Directors
Hotel Monaco
Washington, D.C.
Please visit http://cme.whcenter.org for updated conference information or call 202-877-3200.
Cardiac Surgery Grand Rounds
Weekly, Tuesday, 7 a.m.
CTEC Conference Facility
2 AMA PRA Category 1 Credit
202-801-0905
Cardiology Grand Rounds
Weekly, Tues., 12:30 p.m.
CTEC Conference Theater
1 AMA PRA Category 1 Credit
202-877-8220
Echocardiography Conference
Weekly, Thursday, 7:45 a.m.
CTEC Conference Theater
1.25 AMA PRA Category 1 Credit
202-877-6264
Electrophysiology Core
CurriculumConference
Weekly, Tuesday, 7 a.m. Rm5B3
1 AMA PRA Category 1 Credit
202-877-3951
Electrophysiology
Weekly Conference
Weekly, Wednesday, 4 p.m.
1st & 3rd Wednesdays:
VA Dept. of Medicine
Conference Room(4th Fl.)
2nd & 4th Wednesdays:
Cath Lab Conf. Room(5th Fl.)
1 AMA PRA Category 1 Credit
202-877-6363
Childrens National Medical
Center Pediatric Cardiac
Catheterization Conference
Weekly, Friday, 7:30 a.m.
Childrens Nat. Medical Center
Susan B. Murphy Learning
Center (3rd Fl.)
1 AMA PRA Category 1 Credit
202-476-2020
DERMATOLOGY
National Institutes of Health
Dermatology Grand Rounds
Twice Monthly, 2nd & 4th
Thursday, 8 a.m.
National Institutes of Health,
11S235, Bldg. 10
2 AMA PRA Category 1 Credit
301-496-6383
Washington Hospital Center
Dermatology Grand Rounds
Twice Monthly , Thursday, 8 a.m.
Washington Hospital Center &
Georgetown University Hospital
2 AMA PRA Category 1 Credits
202-877-6654
EMERGENCY MEDICINE
Childrens National Medical
Center Trauma Morbidity &
Mortality Conference
Monthly, 1st Wednesday, 7 a.m.
Childrens Nat. Medical Center
1 AMA PRA Category 1 Credit
202-476-3683
Emergency Department
Grand Rounds
Weekly, Thursday, 9 a.m.
True Auditorium&
Georgetown University
Warwick Evans Conference Rm
4 AMA PRA Category 1 Credit
202-877-8080
Emergency Department
Journal Club
Monthly, 4th Tuesday, 7 p.m.
Various locations
2 AMA PRA Category 1 Credit
202-877-8080
ENDOCRINOLOGY
Endocrine Grand Rounds
Weekly, Tuesday, 8 a.m.
4NWConference Room&
Georgetown University
Warwick Evans Conference Rm
1 AMA PRA Category 1 Credit
202-877-9137
MEDICINE
GI Case Conference
Monthly
Various Restaurant Locations
2 AMA PRA Category 1 Credit
202-829-0170
Medicine Grand Rounds
Weekly, Wednesday, 12:30 p.m.
True Auditorium
1 AMA PRA Category 1 Credit
202-877-6749
MULTIDISCIPLINARY
Calvert Memorial
Grand Rounds
4-6 times annually
Weekly, Tuesday, 5:30 p.m.
Calvert Memorial Hospital
1 AMA PRA Category 1 Credit
410-535-8134
Childrens National Medical
Center Child Injury Seminar
Monthly, 3rd Thursday, 1 p.m.
Childrens National Medical Center
ED Conference Room
1 AMA PRA Category 1 Credit
202-476-3558
MedStar Health Research
Institute Grand Rounds
Monthly, 3rd Friday, noon
CTEC Conference Theater
1 AMA PRA Category 1 Credit
202-877-7164
Multidisciplinary Breast
Cancer Conference
Weekly, Wednesday, 7:30 a.m.
Siegel Auditorium
1 AMA PRA Category 1 Credit
202-877-3914
Multidisciplinary Head
and Neck Tumor Board
Conference
Weekly, Thursday, 4 p.m.
RoomC1-119
1 AMA PRA Category 1 Credit
202-877-9403 or 202-877-6718
Multidisciplinary Sarcoma
Conference
Twice Monthly, Tuesday, 7:30 a.m.
Siegel Auditorium
1.5AMA PRA Category 1 Credits
202-877-8098
NEONATOLOGY
Visiting Lecturer Series in
Perinatal Pediatrics
Twice Monthly, 1st & 2nd
Thursday, 12:30 p.m.
5B3 Conference Room
Morbidity & Mortality
Monthly, 3rd Thursday,
12:30 p.m.
5B3 Conference Room
1 AMA PRA Category 1 Credit
202-877-6527
NEUROLOGY
Cerebrovascular Case
Conference
Twice Monthly, Wednesday, 8 a.m.
Various locations
1 AMA PRA Category 1 Credit
202-877-3154
NEUROSURGERY
Neurosurgery Conference
Weekly, Tuesday, 7:30 a.m.
CTEC Board Room
1 AMA PRA Category 1 Credit
202-877-3154
Neurosurgery Conference
Weekly, Tuesday, 7:30 a.m.
CTEC Board Room
1 AMA PRA Category 1 Credit
202-877-5026
OBSTETRICS/
GYNECOLOGY
OB/GYN Grand Rounds
Weekly, Thursday, 8 a.m.
True Auditorium
Morbidity & Mortality
Weekly, Thursday, 9 a.m.
5B3 Conference Room
Journal Club
Monthly, 1st Thursday, 9:30 a.m.
5B3 Conference Room
Perinatal High Risk
Multidisciplinary Conference
Weekly, Tuesday, 8:00 a.m.
5B-3 Conference Room
1 AMA PRA Category 1 Credit
202-877-9663
ONCOLOGY
Gastrointestinal Oncology
Case Presentations
Twice Monthly, 2nd & 4th
Friday, 8 a.m.
Surgical ClassroomRmG-270
1.5AMA PRA Category 1 Credits
202-877-3908
Oncology Grand Rounds
Weekly, Friday, noon
Siegel Auditorium
1 AMA PRA Category 1 Credit
202-877-2505
Thoracic Oncology
Conference
Weekly, Thursday, 7:30 a.m.
Pathology Conference
Room/Siegel Auditorium
1 AMA PRA Category 1 Credit
202-877-6567
Ophthalmology
Ophthalmology Saturday
Morning Lecture Series
Semi-Monthly, Saturday,
8:30 a.m.
2.5AMA PRA Category 1 Credits
202-877-6159
ORTHOPAEDIC SURGERY
Orthopaedic Surgery
Grand Rounds
Weekly, Monday, 7:30 a.m.
3 NWConference Room
1.5AMA PRA Category 1 Credits
202-877-6664
ORTHOPAEDIC
ONCOLOGY
Orthopaedic Oncology
Preoperative Conference
Weekly, Thursday, 7:30 a.m.
Siegel Auditorium
1.5AMA PRA Category 1 Credits
202-877-8098
PHYSICAL MEDICINE AND
REHABILITATION
NRH Medical Grand Rounds
Weekly, Friday, noon
NRH Auditorium
1 AMA PRA Category 1 Credit
202-877-1657
SURGERY
Burn Center Lunch and Learn
Monthly, Second Thursday, noon,
4B-45
1 AMA PRA Category 1 Credit
202-877-6662
Center for Vascular Surgery
Conference and M&M
Weekly, Thursday 7:30 a.m.
CTEC Conference Theater
2 AMA PRA Category 1 Credits
202-877-8050
General Surgery Orange
TeamTeaching Conference
& Lecture Series
Weekly, Thursday, 8 a.m.
General Surgery Conference Rm
2 AMA PRA Category 1 Credits
202-877-9849
Hepatobiliary Case
Presentations
Monthly, 3rd Friday, 8 a.m.
G-213C Conference Room
1.5AMA PRA Category 1 Credits
202-877-4599
Highly Reliable Surgical Team
Training
Monthly, First Tuesday, 7 a.m.
True Auditorium
1 AMA PRA Category 1 Credit
202-877-0290
Surgery Grand Rounds
and M& M
Weekly, Tuesday, 8 a.m.
True Auditorium
1 AMA PRA Category 1 Credit
202-877-5133
Sunil Madan, MD
Mary-Michael Brown, DPN, RN
ANESTHESIOLOGY
Anesthesiology Clinical
Conference
Weekly, Tuesday, 7 a.m., RmG-200
1 AMA PRA Category 1 Credit
202-877-7504
CARDIOLOGY/
CARDIOVASCULAR
Cardiac Catheterization
Conference & Lecture Series
Weekly, Wednesday, 7:30 a.m.
CTEC Conference Theater
1 AMA PRA Category 1 Credit
202-877-2992
19
JAN/FEB 2012 | PHYSICIAN | MEDSTAR WASHINGTON HOSPITAL CENTER
19
For many college graduates, the
undergraduate experience can often feel
like it flew by. For Wendy Kirkland, MD,
chief resident, Ophthalmology, it wasnt
just a feeling. Dr. Kirkland completed
her undergraduate requirements in just
two years.
I made the decision to become a doctor
when I was 18, Dr. Kirkland recalls.
Medicine is such a long road. Youre a
medical student, then a resident for four
years, then theres often a fellowship. It made
sense to me to accelerate the process as long
as I was certain this is what I wanted to do.
Dr. Kirkland tested out of many required
courses using advanced placement credits,
and enrolled in a six-year BS/MD program
at the University of Akron in
Ohio. She took, on average, 26
credits per semester. Those
semesters were almost entirely
science, and included biology,
physics and chemistry
simultaneously.
But even with a course load that
might keep many students
shackled to a cubby in the
library, Dr. Kirkland was
determined to enjoy the typical
college experience: joining a
sorority, playing club sports and
hanging out with her friends.
When youre in the condensed
program, you live in a dorm, eat
and attend classes with the
same 30 people, which could
feel like high school all over
again. Theres a set standard
curriculum, and you dont
always have the opportunity to
meet new people, Dr. Kirkland
explains. Joining a sorority was
a great way for me to meet new
people. It was really important
for me to get involved with
different groups and activities.
Even for most four year pre-
med students, completing a study abroad
program is usually difficult to manage. Dr.
Kirkland still made it happen, spending a
summer in Florence, Italy studying art
history.
The main question I always get is, Do you
regret doing the accelerated program? says
Dr. Kirkland. I have no regrets. I found the
time to do the things that I really wanted to
do. You have to make most of your
experiences. I ended up doing everything I
wanted to do and more.
I knew I wanted to study abroad and have
that experience. That was a really important
time in my life, Dr. Kirkland says of her
time in Florence. She grew up in Ohio, so
her time in college and medical school did
not feel like such a break from home. Being
so far away, I really felt like I was on my own.
I think it helped me transition into the
person that I am today.
Dr. Kirkland credits her initial pursuit of
medicine to her father, an internist. Dad is
an amazing physician. I look up to him as a
role model. Dr. Kirkland says that when
shes having a bad day or is feeling stressed,
she calls her father. Just hearing how
dedicated he is with his work buoys the
young doctor and inspires her to work at her
best level.
The complexity of ophthalmology attracted
Dr. Kirkland. Ophthalmology has so much
to do with everything in the body; theres
some neurology, some surgery, and some
medicine, notes Dr. Kirkland. It just drew
me in from that aspect. I also had a lot of
great mentors who kept inspiring me.
Cataract surgery has been one part of her
work that Dr. Kirkland finds particularly
rewarding. Its amazing to be able to give
vision to someone who hasnt been able to
see for so long, to help them see their
grandchildren, Dr. Kirkland says. We see
such amazing cases at the Hospital Center.
Patients are so grateful; it gives you the best
feeling, and has been the most rewarding
part of the residency so far.
Dr. Kirkland calls her chief residency year
an amazing, door-opening experience. It
has opened my eyes to the academic side of
residency, and everything that goes on
behind the scenes.
She credits her husband as being her biggest
support system throughout her residency
experience. Its so important to have
someone to lean on, Dr. Kirkland notes.
Dr. Kirkland recently learned she will
continue on in a glaucoma fellowship at
New York Eye and Ear Infirmary next year.
She hopes to return to Washington, D.C.,
someday to join a private practice and give
back to the program that has taught her so
much. n
Maggie Master
Wendy Kirkland, MD
Ophthalmology
18 MEDSTAR WASHINGTON HOSPITAL CENTER | PHYSICIAN | JAN/FEB 2012 18
C H I E F R E S I D E N T S P O T L I G H T
Nicole Proscia, MD &
Scott Dziedzic, MD
Radiology
Nicole Proscia, MD, doesnt like to give her
husband all the credit for steering her toward a specialty in radiology.
In fact, she says she resisted pursuing the specialty at first, because her
future husband was a year ahead of her in medical school, and had
already chosen that field.
Im sure that I influenced her, insists Scott Dziedzic, MD, with a
confident smile. I remember when she was going through her
interests, and I had already done several rotations. I would rave about
how, with radiology, you get to do a little bit of everything. It also felt
like a great fit for both of their personalities and preferences, as
neither loved the operating room.
Despite Dr. Dziedzic leading the way into their eventual specialty,
Dr. Proscia came to radiology on her own terms. The couple may
banter about who turned on whom to radiology, but they both agree
there are big advantages to working in the same field, and in the same
Radiology department at MedStar Washington Hospital Center.
Whats the best part? He brings me Starbucks! Dr. Proscia laughs.
No, wait, can I change my answer? Its really our quiet-time lunch
dates.
Dr. Dziedzic agrees. My favorite part about working with Nicole is
getting a chance to see her during the day. A lot of times its our peace
and quiet time, we can get lunch together or a cup of coffee. Its often
the only time we can quietly have a conversation without Mommy!
Mommy!
The two doctors have two young sons, 3-year-old Harlan and
1-year-old Wade, which means that when theyre not at work, theres
not a lot of one-on-one time, and certainly not a lot of quiet time.
They are time-consuming, says Dr. Dziedzic of their two young
boys. As a family, were so happy, but were also stretched thin. But
theyre so fun. The stuff that comes out of Harlans mouth, its so
funny and innocent and precious at the same time.
The couple met within the first weeks of Dr. Proscias first year of
medical school at New York Medical College, where Dr. Dziedzic was
a second year. He was on the welcoming committeeI think so that
he could meet girls, Dr. Proscia laughs. It worked out well.
Dr. Dziedzic helped Dr. Proscia prepare for her oral exams, as an
upper classman was assigned to every first year. Dr. Dziedzic swears
their pairing was completely coincidental. Im not that devious! he
insists with a laugh. The couple began dating that December, and
were married a week after Dr. Proscia graduated from medical school.
Dr. Dziedzic was already in a residency program at Duke University,
and Dr. Proscia recalls that it was a stressful year, as they waited to see
if shed been matched to Duke (she did). If youre the same year, you
can do a couples match, but since we were one year apart, I had to
put my best foot forward and hope for the best, Dr. Proscia recalls.
We knew we were getting married, and I just thought, Oh gosh,
what if Im not at Duke?
Beyond the occasional quiet lunches and coffee dates, both doctors
agree theres a great advantage to having a trusted colleague just down
the hall, or sometimes in the same reading room.
Dr. Proscia works primarily in womens imaging, but sometimes
finds herself in the body imaging reading room, where Dr. Dziedzic,
the teams primary musculoskeletal radiologist, can usually be found.
Everyone makes the comment Its the Mom-and-Pop radiology
team, Dr. Proscia laughs.
I enjoy being able to see the pathology, to see what the problem is for
a patient, says Dr. Dziedzic. If youre another type of doctor, you
might see 15 patients a day. I get to see 70 different patients and 70
different pathologies: to review it, think about it and then move on
and think about the next interesting pathology.
Both doctors welcome their time together, even the early morning car
pool. He likes to listen to Satellite Radio, she prefers to talk. He
admits, If I havent had my coffee or run that morning, Im not the
most pleasant person to drive in with.
These moments of together time at work and en route have helped
them navigate the constant work of being full-time doctors and
full-time parents. Which leads to Dr. Dziedzics other favorite part
about working with his wife: If she has any questions, Im there to
help. And vice versa. n
Maggie Master
S P O T L I G H T
20 MEDSTAR WASHINGTON HOSPITAL CENTER | PHYSICIAN | JAN/FEB 2012 20
Non-Prot
Organization
U.S. Postage
PAID
MedStar Washington
Hospital Center
110 Irving Street, NW
Washington, DC 20010
Physician
MEDSTAR WASHINGTON HOSPITAL CENTER
MedStar Washington Hospital Center Physicianis
an informative bi-monthly publication for all the members of the
Hospital Center Medical and Dental Staff. It is a forumto report
news of interest to the medical staff, introduce newproviders and
prole current ones, exchange ideas and opinions about subjects
of interest and controversy, and recognize the professional and
personal accomplishments of our practitioners. Its overall goal is to
help foster and celebrate a sense of community among the broad
diversity of the Hospital Center physician membership. The
newsletter is published by the editorial services division of Public
Affairs for the Ofce of Medical Affairs.
MISSIONMedStar Washington Hospital Center is dedicated
to delivering exceptional patient rst health care. We provide the
region with the highest quality and latest medical advances
through excellence in patient care, education and research.
MedStar Washington Hospital Center, a private, not-for-prot
hospital, does not discriminate on grounds of race, religion, color,
gender, physical handicap, national origin or sexual preference.
Visit the hospitals Web page at www.WHCenter.org.
James Jelinek, MD, FACR
Editor
Margo Smith, MD, FACP
Associate Editor
Mark Smith, MD, FACEP
Editor Emeritus
Marge Kumaki
Managing Editor
Marlo Russell
Graphic Design
Micheal Pistole, MD
President,
Medical &Dental Staff
Janis M. Orlowski, MD, MACP
Senior Vice President,
Medical Affairs
and Chief Medical Ofcer
Ty Kennon
Vice President, Public Affairs
and Marketing
JohnSullivan, President, MedStar Washington Hospital Center
Dennis R. Wraase, Chairman of the Board
MedStar Washington Hospital Center
KennethA. Samet, FACHE, President and CEO, MedStar Health
Editorial Board Members
John Buek, MD Jeffrey
Dubin, MD Zayd Eldadah,
MD, PhD Philip Fidler, MD
Cheryl Iglesia, MD
Karen M. Johnson, MD
Geoffrey Kaung, MD
Robert Lowery, MD
Adedamola Omogbenin, MD
Stephen Peterson, MD
Micheal Pistole, MD Kevin
Reed, MD Jen Remington
George Ruiz, MD Marc
Schlosberg, MD Douglas
Snyder, MD
Contributing Writers
Catherine Avery
Norma Babington
Lynn Cantwell
Maggie Master
JimParsons
C O N TA C T I N F O R MAT I O N
James S. Jelinek, MD, FACR
Editor 202-877-6088
James.S.Jelinek@MedStar.net
Margo Smith, MD, FACP
Associate Editor 202-877-7164
Margo.A.Smith@MedStar.net
Marge Kumaki
Managing Editor 202-877-8530
Marge.Kumaki@MedStar.net
techniques, the use of heart assist devices
and access to continuous dialysis.
The public is expecting better quality care at
lower costs. Health care demands are growing
dramatically, while the number of
practitioners is staying flat or shrinking. Our
society faces a national challengein the
final six months of life, incredible medical
resources are expended to extend life.
In critical care, we struggle mightily to
understand how to best help our patients
improve, and to wisely understand when
they cant. Most heal and return home, but
we need to reduce those interventions that
wont help a patient recover, and assist
families and practitioners to recognize when
we should begin to shift to comfort care.
Thats where our clinical ethicists and
palliative care team provide an invaluable
service.
Im proud of the critical care services we
provide. I believe we offer unique services to
patients, and to the programs within the
hospital that depend on critical care. The
beauty of our critical care team is that we
have the knowledge and wisdom to astutely
monitor and care for patients who have or
are at risk for multisystem organ
dysfunction. n
MedStar Washington
Hospital Centers critical care units are
large, among the top five percent in the
nation. We see more than 7,000 ICU
patients each year, who occupy 20,000 bed
days. Eight units include coronary care and
neonatal care, with the remainder split
between medical and surgical units, the
majority of which are surgical beds. Our
adult units care for those following elective
surgery and medical, cardiologic or surgical
emergencies such as trauma and burns.
Our organized critical care services began
more than 30 years ago, and we were one of
the forerunners in the nation. We have
incorporated intensivists into our teams
from the start, and partner with specially
trained nurses, respiratory therapists,
pharmacists, nutritionists, physician
assistants and nurse practitioners, and we
train residents and fellows.
Our adults are of all ages, many with
complex, chronic diseases that result in
greater challenges to help them recover. Ive
identified two major evolutions in critical
care since we started: the development of
organized, specialized critical care teams,
and a tremendous expansion in diagnostic
and therapeutic modalities. At the Hospital
Center, we offer specialized treatments, such
as the management of increased intracranial
pressure, advanced ventilatory and circulatory
From the Desk of
Arthur St. Andre, MD, FCCM
Director, Surgical Critical Care Services
P H Y S I C I A N S P E R S P E C T I V E
S-ar putea să vă placă și
- Soap Note 5.0Document4 paginiSoap Note 5.0Paulus IskandarÎncă nu există evaluări
- Kingston Hospital Blue Book 2019Document207 paginiKingston Hospital Blue Book 2019Chris Jardine LiÎncă nu există evaluări
- Nursing Research Paper SampleDocument4 paginiNursing Research Paper Samplefyrj7h9z100% (1)
- ... Advocating For Those With Acute Disseminated Encephalomyelitis, Neuromyelitis Optica, Optic Neuritis and Transverse MyelitisDocument12 pagini... Advocating For Those With Acute Disseminated Encephalomyelitis, Neuromyelitis Optica, Optic Neuritis and Transverse MyelitisTransverse Myelitis AssociationÎncă nu există evaluări
- PHD Thesis Topics Public HealthDocument6 paginiPHD Thesis Topics Public Healthbsgnqj4n100% (2)
- Research Paper Topics in Clinical PharmacyDocument7 paginiResearch Paper Topics in Clinical Pharmacyyvunfevgf100% (1)
- Dissertation Cardiac NursingDocument8 paginiDissertation Cardiac NursingWriteMyPersuasivePaperGlendale100% (1)
- Rguhs Thesis Topics PDFDocument4 paginiRguhs Thesis Topics PDFihbjtphig100% (2)
- Thesis Topics Emergency MedicineDocument4 paginiThesis Topics Emergency Medicinerikkiwrightarlington100% (1)
- Anaesthesia Thesis Topics RguhsDocument5 paginiAnaesthesia Thesis Topics Rguhsb0sus1hyjaf2100% (2)
- Thesis Topics in General Surgery DownloadDocument4 paginiThesis Topics in General Surgery Downloadjqcoplhld100% (1)
- Thesis Topics Ophthalmology RguhsDocument4 paginiThesis Topics Ophthalmology Rguhsgjh2y8s8100% (2)
- Rguhs Thesis Topics in General Medicine PDFDocument7 paginiRguhs Thesis Topics in General Medicine PDFtracyjimenezstamford100% (2)
- Rguhs Thesis TopicsDocument6 paginiRguhs Thesis TopicsAshley Carter100% (2)
- Health Informatics Dissertation TopicsDocument5 paginiHealth Informatics Dissertation TopicsWriteMyNursingPaperTopeka100% (1)
- MEDICAL BUZZ VOLUME 7 Final Edition - Compressed PDFDocument28 paginiMEDICAL BUZZ VOLUME 7 Final Edition - Compressed PDFJoelÎncă nu există evaluări
- Nursing Thesis Topic IdeasDocument4 paginiNursing Thesis Topic Ideasgbwav8m4100% (2)
- Dental Thesis Topics RguhsDocument5 paginiDental Thesis Topics Rguhspatricemillertulsa100% (1)
- Pediatric Cardiology Thesis TopicsDocument4 paginiPediatric Cardiology Thesis Topicspzblktgld100% (2)
- Rguhs Thesis 2013Document8 paginiRguhs Thesis 2013fc51eh59100% (2)
- Dissertation in Internal MedicineDocument7 paginiDissertation in Internal MedicineWhereToBuyPapersUK100% (1)
- Health Dissertation TopicsDocument6 paginiHealth Dissertation TopicsUK100% (1)
- Thesis Topics Related To Medical Surgical NursingDocument5 paginiThesis Topics Related To Medical Surgical Nursingubkciwwff100% (2)
- Nurse Practitioner Dissertation TopicsDocument8 paginiNurse Practitioner Dissertation TopicsWriteMyPersuasivePaperGlendale100% (1)
- Rguhs Dissertation SynopsisDocument4 paginiRguhs Dissertation SynopsisHelpWithCollegePapersSingapore100% (1)
- Ultrasound Dissertation IdeasDocument4 paginiUltrasound Dissertation IdeasCustomPapersReviewSingapore100% (1)
- Dissertation Topics General SurgeryDocument5 paginiDissertation Topics General SurgeryWhereCanIFindSomeoneToWriteMyCollegePaperCanada100% (1)
- Diagnostic Radiography Dissertation QuestionsDocument4 paginiDiagnostic Radiography Dissertation QuestionsBestOnlinePaperWritersBillings100% (1)
- Radiodiagnosis Dissertation TopicsDocument5 paginiRadiodiagnosis Dissertation TopicsHelpWithPapersScottsdale100% (1)
- Nuclear Medicine Research Paper TopicsDocument6 paginiNuclear Medicine Research Paper Topicsxfdacdbkf100% (1)
- Graduation Speech Sacred Hear Truth AnnDocument12 paginiGraduation Speech Sacred Hear Truth AnnJecintha JosephineÎncă nu există evaluări
- Wound Care ThesisDocument4 paginiWound Care Thesiscandacedaiglelafayette100% (2)
- Thesis Topics Medical Surgical NursingDocument6 paginiThesis Topics Medical Surgical NursingPaySomeoneToWritePaperCanada100% (2)
- Fall 2014 Communique by Anesthesia Business ConsultantsDocument28 paginiFall 2014 Communique by Anesthesia Business ConsultantsAnesthesia Business ConsultantsÎncă nu există evaluări
- Dissertation On Community Health NursingDocument6 paginiDissertation On Community Health NursingBuyCollegePapersClearwater100% (1)
- Emergency Medicine Dissertation TopicsDocument8 paginiEmergency Medicine Dissertation TopicsBuyCollegePaperSingapore100% (1)
- Thesis Statement For Healthcare ManagementDocument4 paginiThesis Statement For Healthcare ManagementMonica Franklin100% (2)
- Oral Medicine Dissertation TopicsDocument6 paginiOral Medicine Dissertation TopicsWriteMyPersuasivePaperSingapore100% (1)
- Stress Management Thesis in PhilippinesDocument7 paginiStress Management Thesis in Philippinesafjrooeyv100% (2)
- Thesis Community MedicineDocument5 paginiThesis Community Medicinemelissadudassouthbend100% (2)
- Hospital Management Thesis PDFDocument4 paginiHospital Management Thesis PDFfc34qtwg100% (2)
- Thesis Cancer HospitalDocument7 paginiThesis Cancer HospitalCollegePaperWritingServiceCanada100% (2)
- Health Economics PHD Thesis TopicsDocument5 paginiHealth Economics PHD Thesis TopicsBuySchoolPapersSingapore100% (1)
- Journal: Complementary & Alternative MedicinesDocument0 paginiJournal: Complementary & Alternative MedicinesEmanuel BonatÎncă nu există evaluări
- Thesis Topics in Child Health NursingDocument5 paginiThesis Topics in Child Health NursingCarrie Tran100% (2)
- Research Paper On MhealthDocument4 paginiResearch Paper On Mhealtht1tos1z0t1d2100% (1)
- Journal of The California Dental Association Nov 2007Document41 paginiJournal of The California Dental Association Nov 2007gerardo_ureñaÎncă nu există evaluări
- Newsletter 6Document4 paginiNewsletter 6api-139326359Încă nu există evaluări
- Diskusi Dan Keterbatasan StudiDocument11 paginiDiskusi Dan Keterbatasan StudiKelas SAP2018Încă nu există evaluări
- Nursing Research Paper TemplateDocument7 paginiNursing Research Paper Templateaflbqewzh100% (1)
- Heribert Reiter DissertationDocument6 paginiHeribert Reiter DissertationCustomWrittenPapersCanada100% (1)
- Thesis Nursing TopicsDocument7 paginiThesis Nursing Topicscynthiasmithmanchester100% (2)
- Thesis Topics Community MedicineDocument7 paginiThesis Topics Community MedicineMonique Carr100% (1)
- Mba Thesis Topics in Health CareDocument8 paginiMba Thesis Topics in Health Caresuejonessalem100% (2)
- Dissertation Topics in HealthcareDocument4 paginiDissertation Topics in HealthcareBuyAPaperForCollegeSingapore100% (1)
- Rguhs Dissertation Topics SurgeryDocument8 paginiRguhs Dissertation Topics Surgerytuocowrothin1972100% (1)
- Research Paper Health Care ManagementDocument5 paginiResearch Paper Health Care Managementefgncpe8100% (1)
- Stemedix Announces The Grand Opening of Their New St. Petersburg FacilityDocument2 paginiStemedix Announces The Grand Opening of Their New St. Petersburg FacilityPR.comÎncă nu există evaluări
- Nursing Thesis TopicsDocument6 paginiNursing Thesis TopicsBuyThesisPaperSingapore100% (1)
- Thesis RguhsDocument5 paginiThesis Rguhsdianamarquezalbuquerque100% (2)
- Dissertation Topics On Community Health NursingDocument4 paginiDissertation Topics On Community Health NursingWhatAreTheBestPaperWritingServicesCanada100% (1)
- د. هالة Dermatitis-1 (Muhadharaty)Document7 paginiد. هالة Dermatitis-1 (Muhadharaty)adwÎncă nu există evaluări
- Drug InteractionDocument151 paginiDrug Interactionapi-3724213100% (1)
- Pyogenic GranulomaDocument6 paginiPyogenic GranulomaRini TiaraÎncă nu există evaluări
- Algorithm GERD Primary Care Pathway Ahs SCN DH 2020 15262Document7 paginiAlgorithm GERD Primary Care Pathway Ahs SCN DH 2020 15262Mihaela ShimanÎncă nu există evaluări
- 1026 FullDocument5 pagini1026 FullMuhammad Yufimar Rizza FadilahÎncă nu există evaluări
- Laryngopharyngeal Reflux and Functional Laryngeal Disorder: Perspective and Common Practice of The General GastroenterologistDocument9 paginiLaryngopharyngeal Reflux and Functional Laryngeal Disorder: Perspective and Common Practice of The General GastroenterologistKenzi A HasyaputraÎncă nu există evaluări
- MS SDS SR Repo Ort: Name of S Model SampleDocument7 paginiMS SDS SR Repo Ort: Name of S Model SampleCamilo WispÎncă nu există evaluări
- Essential Intrapartum and Newborn Care: Health Science Department Southway College of TechnologyDocument3 paginiEssential Intrapartum and Newborn Care: Health Science Department Southway College of TechnologyRowena AngelesÎncă nu există evaluări
- SSNHL SsoDocument3 paginiSSNHL SsoMuhammad HanifÎncă nu există evaluări
- Amphastar Cortrosyn-11-09Document2 paginiAmphastar Cortrosyn-11-09Shivanya SharmaÎncă nu există evaluări
- Immunofluorescence Techniques: Ian D. Odell and Deborah CookDocument4 paginiImmunofluorescence Techniques: Ian D. Odell and Deborah CookbalamurugantÎncă nu există evaluări
- Surgery OSCE QuestionsDocument27 paginiSurgery OSCE QuestionsDineish MurugaiahÎncă nu există evaluări
- Vein Artery Capillary: Thin Wall Wide Lumen Valve Thick Wall Narrow Lumen One Cell Thick WallDocument1 paginăVein Artery Capillary: Thin Wall Wide Lumen Valve Thick Wall Narrow Lumen One Cell Thick WallHuiso RohÎncă nu există evaluări
- The Orthodontic Mini-Implants Failures Based On Patient Outcomes: Systematic ReviewDocument13 paginiThe Orthodontic Mini-Implants Failures Based On Patient Outcomes: Systematic ReviewKristin HalimÎncă nu există evaluări
- 26 - Nonsurgical Treatment of Peyronies DiseaseDocument4 pagini26 - Nonsurgical Treatment of Peyronies DiseaseNunuh SulaemanÎncă nu există evaluări
- UrosepsisDocument22 paginiUrosepsisWita Ferani KartikaÎncă nu există evaluări
- Clinical Symptom Score of The Japanese Orthopaedic Association PDFDocument3 paginiClinical Symptom Score of The Japanese Orthopaedic Association PDFJoanne NgimÎncă nu există evaluări
- Jemds Title PDocument1 paginăJemds Title PKriti KumariÎncă nu există evaluări
- Endocrine SystemDocument35 paginiEndocrine SystemLinkÎncă nu există evaluări
- Integrated Vector Control ProgramDocument35 paginiIntegrated Vector Control ProgramKeerthi VasanÎncă nu există evaluări
- Grade 9 Biology - Lesson Note April 8,2020Document10 paginiGrade 9 Biology - Lesson Note April 8,2020micahxÎncă nu există evaluări
- v20 n4Document223 paginiv20 n4Sivanantham KrishnamoorthiÎncă nu există evaluări
- NCP BaiaeDocument7 paginiNCP BaiaeJonathan Delos ReyesÎncă nu există evaluări
- Corticosteroids and Associated DiseasesDocument76 paginiCorticosteroids and Associated DiseasesALNAKIÎncă nu există evaluări
- NCP - Activity IntoleranceDocument5 paginiNCP - Activity IntolerancePrincess Alane MorenoÎncă nu există evaluări
- NyeriDocument33 paginiNyeriAndriHernadiÎncă nu există evaluări
- Tabel IcdDocument214 paginiTabel IcdSusilo HendroÎncă nu există evaluări
- Case Scenario/Situation Answer/Explanation: NCM 101 RLE - Health AssessmentDocument2 paginiCase Scenario/Situation Answer/Explanation: NCM 101 RLE - Health AssessmentmaryÎncă nu există evaluări