S-ar putea să vă placă și
- Normal Lab Values GuideDocument2 paginiNormal Lab Values GuideItharshan Indreswaran83% (18)
- Practise Questions Keith & Moore 5th Edition - Should ReadDocument113 paginiPractise Questions Keith & Moore 5th Edition - Should ReadAmirsalar Eslami83% (6)
- Pharmacology - Mnemonics PDFDocument140 paginiPharmacology - Mnemonics PDFItharshan Indreswaran76% (17)
- Pharmacology - Mnemonics PDFDocument140 paginiPharmacology - Mnemonics PDFItharshan Indreswaran76% (17)
- Poster2 Arrhythmia Recognition eDocument1 paginăPoster2 Arrhythmia Recognition eItharshan IndreswaranÎncă nu există evaluări
- Respiratory Failure MCQ QuestionsDocument5 paginiRespiratory Failure MCQ QuestionsChikezie Onwukwe67% (3)
- 1 Medicine MCQs - CNSDocument10 pagini1 Medicine MCQs - CNSDiwakesh C B80% (5)
- 2009 Grainger & Allison'sDocument409 pagini2009 Grainger & Allison'sGabriel Callupe100% (4)
- Pulmon Ology MCQ SDocument280 paginiPulmon Ology MCQ SSai ShankerÎncă nu există evaluări
- MCQS OF RESPIRATORY SYSTEM - DetailDocument3 paginiMCQS OF RESPIRATORY SYSTEM - Detailhashmat aliÎncă nu există evaluări
- MCQs PulmonologyDocument2 paginiMCQs PulmonologySadia Batool86% (7)
- Chapter 25 PLEURAL DISEASEDocument8 paginiChapter 25 PLEURAL DISEASEZahra Margrette SchuckÎncă nu există evaluări
- Respiratory Physiology AnswersDocument4 paginiRespiratory Physiology AnswersRamya100% (2)
- General Practitioner - Pulmonology MCQsDocument37 paginiGeneral Practitioner - Pulmonology MCQsAsif Newaz100% (7)
- Multiple Choice Questions in Ophthalmic and NeuroanatomyDe la EverandMultiple Choice Questions in Ophthalmic and NeuroanatomyÎncă nu există evaluări
- Herbal Approach to Managing Polycystic Ovarian Syndrome (PCOS) SymptomsDocument1 paginăHerbal Approach to Managing Polycystic Ovarian Syndrome (PCOS) SymptomsItharshan IndreswaranÎncă nu există evaluări
- SP42 Thoracentesis (Adult)Document7 paginiSP42 Thoracentesis (Adult)Adam HuzaibyÎncă nu există evaluări
- 8.11.08 Davis-Hovda. TB PleurisyDocument13 pagini8.11.08 Davis-Hovda. TB Pleurisyawaniedream8391Încă nu există evaluări
- Pulmonology MCQsDocument49 paginiPulmonology MCQsaliakbar178100% (1)
- Pneumology 2018Document16 paginiPneumology 2018Kris100% (1)
- BB Sample Exam MCQDocument15 paginiBB Sample Exam MCQbobobo96Încă nu există evaluări
- Pulmonary Medicine 1Document28 paginiPulmonary Medicine 1Gloria JaisonÎncă nu există evaluări
- Pulmonology: The Cells of The Bronchial Epithelium, LeucocytesDocument64 paginiPulmonology: The Cells of The Bronchial Epithelium, LeucocytesSk Chaudhry100% (1)
- Lung Disease Diagnosis and Treatment Multiple Choice QuestionsDocument17 paginiLung Disease Diagnosis and Treatment Multiple Choice QuestionsOsman Somi100% (1)
- Pulmonology MRE CH 278-287Document5 paginiPulmonology MRE CH 278-287herrerachaimÎncă nu există evaluări
- Med Respi T&D QuestionsDocument14 paginiMed Respi T&D QuestionsD PatelÎncă nu există evaluări
- Wiki Resp Mcqs ExplainedDocument7 paginiWiki Resp Mcqs ExplainedArvinth Guna SegaranÎncă nu există evaluări
- Lung MCQDocument7 paginiLung MCQArvinth Guna Segaran100% (2)
- Path Lung McqsDocument24 paginiPath Lung McqsShafaque IrfanÎncă nu există evaluări
- Respiratory Medicine 151 200Document31 paginiRespiratory Medicine 151 200Ahmed Kh. Abu Warda100% (2)
- MCQ-Chronic Obstructive Pulmonary DiseaseDocument3 paginiMCQ-Chronic Obstructive Pulmonary DiseaseMittulÎncă nu există evaluări
- RS MCQsDocument2 paginiRS MCQsraed faisalÎncă nu există evaluări
- Pulmonology Review: Key Topics in Lung Disease ManagementDocument23 paginiPulmonology Review: Key Topics in Lung Disease ManagementAsif Newaz100% (1)
- RespiratoryDocument57 paginiRespiratoryMuhammad Javed GabaÎncă nu există evaluări
- MED2031 Mid Semester Practice Exam Respiratory Physiology QuestionsDocument29 paginiMED2031 Mid Semester Practice Exam Respiratory Physiology QuestionsTyler VargasÎncă nu există evaluări
- Respiratory MCQDocument10 paginiRespiratory MCQSyeda Aroosa Abbas Naqvi100% (1)
- Pleural MCQS MedicineDocument17 paginiPleural MCQS MedicineCheryls Raju100% (1)
- Respiratory MCQs LJDocument7 paginiRespiratory MCQs LJfjghÎncă nu există evaluări
- Respiration MCQs (2016), Dr. Ahmad AlarabiDocument7 paginiRespiration MCQs (2016), Dr. Ahmad AlarabiTofik Mohammed100% (1)
- TB & PneumoniaDocument16 paginiTB & PneumoniacseÎncă nu există evaluări
- Exam 2Document45 paginiExam 2dkmm100% (1)
- Liver Disease Signs & SymptomsDocument5 paginiLiver Disease Signs & SymptomsCHRISTOPHER OWUSU ASAREÎncă nu există evaluări
- TUBERCLUOSIS MCQS, ZSMU, UkraineDocument26 paginiTUBERCLUOSIS MCQS, ZSMU, UkraineDrRaghavender Reddy100% (1)
- 8th Finals McqsDocument28 pagini8th Finals McqsMuhammad Uzair GujjarÎncă nu există evaluări
- Shams Pulmonary Quiz 1Document9 paginiShams Pulmonary Quiz 1tylermedÎncă nu există evaluări
- Physio MCQ’s on Respiration, Deep Sea Diving & AviationDocument2 paginiPhysio MCQ’s on Respiration, Deep Sea Diving & Aviationbushra100% (3)
- CVS Irfan HabibDocument6 paginiCVS Irfan HabibPardeep Dhurgesh Nkh RatananiÎncă nu există evaluări
- 1017MSC T6 Respiratory Revision Sheets & Answers 2011Document23 pagini1017MSC T6 Respiratory Revision Sheets & Answers 2011MobarobberÎncă nu există evaluări
- MCQ RespiratoryDocument6 paginiMCQ Respiratorynurulhudaabdulmuiez100% (2)
- MCQ Part 1 2005 "Example Questions"Document3 paginiMCQ Part 1 2005 "Example Questions"RayC1977Încă nu există evaluări
- Pharm Resp Mcqs PDFDocument8 paginiPharm Resp Mcqs PDFVikashgtmÎncă nu există evaluări
- Mcqs Resp 3Document4 paginiMcqs Resp 3jhhÎncă nu există evaluări
- Respiratory System Functions and ProcessesDocument9 paginiRespiratory System Functions and ProcessesIan MatatulaÎncă nu există evaluări
- My Masterclass Create Exam My History My DetailsDocument100 paginiMy Masterclass Create Exam My History My DetailsMuntasir BashirÎncă nu există evaluări
- Respiratory System Study GuideDocument13 paginiRespiratory System Study GuidebisnumÎncă nu există evaluări
- Mcqs IV Year Students SurgeryDocument38 paginiMcqs IV Year Students SurgeryAbdimajiidÎncă nu există evaluări
- Mycobacterium tuberculosis Multiple Choice QuestionsDocument31 paginiMycobacterium tuberculosis Multiple Choice QuestionsSp PpvÎncă nu există evaluări
- General Medicine - Surgery IV YearDocument40 paginiGeneral Medicine - Surgery IV YearCynthia GÎncă nu există evaluări
- Respiratory System BCQsDocument31 paginiRespiratory System BCQsSajid AliÎncă nu există evaluări
- Respirology OXF.: I. Common Respiratory PresentationsDocument17 paginiRespirology OXF.: I. Common Respiratory PresentationsFarah FarahÎncă nu există evaluări
- Tropical MCQS: C. Visceral LeishmaniasisDocument29 paginiTropical MCQS: C. Visceral Leishmaniasisساره ابوالقاسمÎncă nu există evaluări
- MCQS With KEY - PAEDSDocument7 paginiMCQS With KEY - PAEDSSiraj Ul IslamÎncă nu există evaluări
- Respiratory MCQDocument3 paginiRespiratory MCQMarjina Khatoon NipuÎncă nu există evaluări
- MCQ RespiratoryDocument6 paginiMCQ Respiratoryalemante100% (2)
- Cvs MCQDocument52 paginiCvs MCQMiracle For NursesÎncă nu există evaluări
- MCQsDocument21 paginiMCQsZweÎncă nu există evaluări
- Pediatric Respiratory DiseaseDocument5 paginiPediatric Respiratory DiseaseMuhammad Noor BumiputraÎncă nu există evaluări
- End Blok Respi SoalDocument6 paginiEnd Blok Respi Soalanz_4191Încă nu există evaluări
- CRT Exam Review Guide Chapter 3Document10 paginiCRT Exam Review Guide Chapter 3Dharlyn MungcalÎncă nu există evaluări
- Pharmacology - Anti-Inflammatory Drugs - Corticosteroid, NSAID, Leukotriene (Eicosanoids)Document9 paginiPharmacology - Anti-Inflammatory Drugs - Corticosteroid, NSAID, Leukotriene (Eicosanoids)Itharshan IndreswaranÎncă nu există evaluări
- Carcinogens - Carcinogens by Sites of Body (IARC) PDFDocument1 paginăCarcinogens - Carcinogens by Sites of Body (IARC) PDFItharshan IndreswaranÎncă nu există evaluări
- Gastroeneteritis - Pediatrics (Nelson's)Document20 paginiGastroeneteritis - Pediatrics (Nelson's)Itharshan IndreswaranÎncă nu există evaluări
- Abdomen Diagnoses PDFDocument2 paginiAbdomen Diagnoses PDFLaura Lopez RocaÎncă nu există evaluări
- Cardiovascular Regulation - PhysiologyDocument9 paginiCardiovascular Regulation - PhysiologyItharshan IndreswaranÎncă nu există evaluări
- Bradycardia PDFDocument1 paginăBradycardia PDFItharshan IndreswaranÎncă nu există evaluări
- Asthma (Acute) Management - Children (Pediatrics)Document2 paginiAsthma (Acute) Management - Children (Pediatrics)Itharshan IndreswaranÎncă nu există evaluări
- Circulatory System - Arterial & Venous TreesDocument28 paginiCirculatory System - Arterial & Venous TreesItharshan IndreswaranÎncă nu există evaluări
- Amenorrhea - Algorithm & DifferentialsDocument9 paginiAmenorrhea - Algorithm & DifferentialsItharshan IndreswaranÎncă nu există evaluări
- Spirometry Curve Errors Correction PDFDocument1 paginăSpirometry Curve Errors Correction PDFItharshan IndreswaranÎncă nu există evaluări
- Rash - Severely Ill (Differentials) PDFDocument11 paginiRash - Severely Ill (Differentials) PDFItharshan IndreswaranÎncă nu există evaluări
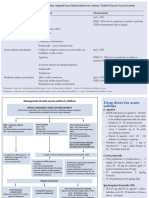
- Acute Severe Asthma Hospital ManagementDocument1 paginăAcute Severe Asthma Hospital ManagementItharshan IndreswaranÎncă nu există evaluări
- Acute Severe Asthma Hospital ManagementDocument1 paginăAcute Severe Asthma Hospital ManagementItharshan IndreswaranÎncă nu există evaluări
- Martyrs Park PDFDocument5 paginiMartyrs Park PDFItharshan IndreswaranÎncă nu există evaluări
- Martyrs Park PDFDocument5 paginiMartyrs Park PDFItharshan IndreswaranÎncă nu există evaluări
- Introduction To Chinese Society and CultureDocument5 paginiIntroduction To Chinese Society and CultureItharshan IndreswaranÎncă nu există evaluări
- PE - Quizlet - Flash Card (Table)Document6 paginiPE - Quizlet - Flash Card (Table)Itharshan IndreswaranÎncă nu există evaluări
- Martyrs ParkDocument6 paginiMartyrs ParkItharshan IndreswaranÎncă nu există evaluări
- Chapter 22Document14 paginiChapter 22Itharshan IndreswaranÎncă nu există evaluări
- Classification of Cardiac MurmursDocument1 paginăClassification of Cardiac MurmursItharshan IndreswaranÎncă nu există evaluări
- Abdominal Aorta SonogramDocument3 paginiAbdominal Aorta SonogramItharshan IndreswaranÎncă nu există evaluări
- Introduction in Human ParasitologyDocument53 paginiIntroduction in Human ParasitologyItharshan IndreswaranÎncă nu există evaluări
- Pharmacology: For Health Science StudentsDocument211 paginiPharmacology: For Health Science StudentssafibayÎncă nu există evaluări
- General PathologyDocument261 paginiGeneral PathologyHanif SharÎncă nu există evaluări
- NBME Samples Qs - PathologyDocument7 paginiNBME Samples Qs - PathologyAli AlshehhiÎncă nu există evaluări
- Tindakan TorakosentesisDocument15 paginiTindakan TorakosentesisSheilla ElfiraÎncă nu există evaluări
- Differential DiagnosisDocument5 paginiDifferential DiagnosisChristie LucasÎncă nu există evaluări
- Chest Tube SizeDocument10 paginiChest Tube SizeilpollolocoÎncă nu există evaluări
- Kegawatan Respirasi Pada Keganasan Rongga ToraksDocument57 paginiKegawatan Respirasi Pada Keganasan Rongga ToraksChristian HarnatÎncă nu există evaluări
- DX Imaging 1 MT and FinalDocument24 paginiDX Imaging 1 MT and FinalRaymondÎncă nu există evaluări
- TimeoutDocument10 paginiTimeoutDuskoÎncă nu există evaluări
- Discharge Plan Patient Teaching Pleural Effusion CastleDocument6 paginiDischarge Plan Patient Teaching Pleural Effusion Castleapi-341263362100% (2)
- Radiology CWRU Medical Student Elective Week 1Document112 paginiRadiology CWRU Medical Student Elective Week 1Yopi SimargiÎncă nu există evaluări
- ThoracentesisDocument36 paginiThoracentesisMarivic DianoÎncă nu există evaluări
- Dapus Efusi Pleura OsteosarcomaDocument3 paginiDapus Efusi Pleura OsteosarcomaKhalila IzdiharÎncă nu există evaluări
- Underwater Seal Chest DrainageDocument22 paginiUnderwater Seal Chest DrainageRegina SeptianiÎncă nu există evaluări
- Case Study For Pleural-EffusionDocument10 paginiCase Study For Pleural-EffusionGabbii CincoÎncă nu există evaluări
- Narrative PathophysiologyDocument18 paginiNarrative PathophysiologyNica Georgelle Maniego SamonteÎncă nu există evaluări
- Nursing Managment of Chest Tubes: by Alice Leung RN, BSN, PCCNDocument55 paginiNursing Managment of Chest Tubes: by Alice Leung RN, BSN, PCCNFrancis Xavier S. Mendez0% (1)
- Brief Description: Pleural EffusionDocument3 paginiBrief Description: Pleural EffusionJessica CatacutanÎncă nu există evaluări
- Assisting The Patient Undergoing Thoracentesis PDFDocument2 paginiAssisting The Patient Undergoing Thoracentesis PDFSITTIE JOBAISAH TOMINAMAN ALIÎncă nu există evaluări
- Lesson Plan On Pleural EffusionDocument9 paginiLesson Plan On Pleural EffusionAnonymous 0C4OZmR100% (1)
- Pleural Effusion Case StudyDocument31 paginiPleural Effusion Case StudyHomework PingÎncă nu există evaluări
- PleuritisDocument32 paginiPleuritisrianiÎncă nu există evaluări
- Clinico Radiological ConferenceDocument67 paginiClinico Radiological ConferenceSharmaine Margaret LeeÎncă nu există evaluări
- Respiratory Conditions and FunctionsDocument120 paginiRespiratory Conditions and Functionsrosalyn gaboniÎncă nu există evaluări
- Pleural DiseasesDocument52 paginiPleural DiseasesAmolkumar W DiwanÎncă nu există evaluări
- Basic Chest UltrasoundDocument60 paginiBasic Chest UltrasoundAdriana Villarreal100% (1)
- Go With The Flow of Chest Tube Therapy: by Arlene M. Coughlin, RN, MSN, and Carolyn Parchinsky, RN, MADocument14 paginiGo With The Flow of Chest Tube Therapy: by Arlene M. Coughlin, RN, MSN, and Carolyn Parchinsky, RN, MAhady920100% (1)