S-ar putea să vă placă și
- Allah (SWT) Is The Best of Those Who PlotDocument4 paginiAllah (SWT) Is The Best of Those Who PlotIffatNaeemÎncă nu există evaluări
- Hypothyroidism AIM 2009Document16 paginiHypothyroidism AIM 2009IffatNaeem100% (1)
- Non-Thyroidal Illness Endo Clin NA 2007Document16 paginiNon-Thyroidal Illness Endo Clin NA 2007IffatNaeemÎncă nu există evaluări
- MGMT Subclinical HypothyroidismDocument4 paginiMGMT Subclinical HypothyroidismIffatNaeemÎncă nu există evaluări
- Approach To NTMNG Jcem 2011Document11 paginiApproach To NTMNG Jcem 2011IffatNaeemÎncă nu există evaluări
- Amiodarone & Thyroid Disease JCEM 2010Document8 paginiAmiodarone & Thyroid Disease JCEM 2010IffatNaeemÎncă nu există evaluări
- Yale Insulin Infusion ProtocolDocument2 paginiYale Insulin Infusion ProtocolIffatNaeemÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- SOAP FormatDocument2 paginiSOAP FormatFarooq ShahÎncă nu există evaluări
- Plant Usage in Protecting The Farm Animal Health - V. Davidović, M. Joksimović Todorović, B. Stojanović, R. RelićDocument12 paginiPlant Usage in Protecting The Farm Animal Health - V. Davidović, M. Joksimović Todorović, B. Stojanović, R. RelićCk_psihÎncă nu există evaluări
- List of Books To Be Used For Rasashastra Data CollectionDocument1 paginăList of Books To Be Used For Rasashastra Data CollectionMikel MillerÎncă nu există evaluări
- Work Work - Life Balance Life Balance ƛ ƛ Understanding The Complex World Understanding The Complex WorldDocument22 paginiWork Work - Life Balance Life Balance ƛ ƛ Understanding The Complex World Understanding The Complex WorldKrishan SainiÎncă nu există evaluări
- Bells That Ring - Proctor, K. (1997)Document4 paginiBells That Ring - Proctor, K. (1997)elaineÎncă nu există evaluări
- Scorpion Envenomation Causing Neuromuscular Toxicity (United States, Mexico, Central America, and Southern Africa) - UpToDateDocument28 paginiScorpion Envenomation Causing Neuromuscular Toxicity (United States, Mexico, Central America, and Southern Africa) - UpToDatejoaoalmeida_1955100% (1)
- Brand Name - Generic NameDocument6 paginiBrand Name - Generic Namejonette carataoÎncă nu există evaluări
- Cardiogenic ShockDocument27 paginiCardiogenic ShockMuhammad Ikbar100% (1)
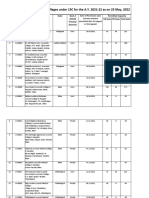
- List of Permitted Ayurveda Colleges For The A.Y. 2021-22 Till 06.05.2022Document52 paginiList of Permitted Ayurveda Colleges For The A.Y. 2021-22 Till 06.05.2022Re Ed EstÎncă nu există evaluări
- Bereavement and Autism: A Universal Experience With Unique ChallengesDocument11 paginiBereavement and Autism: A Universal Experience With Unique ChallengesBrian A. Wong100% (1)
- CGHS Rates 2014 - AhmadabadDocument72 paginiCGHS Rates 2014 - AhmadabadJayakrishna ReddyÎncă nu există evaluări
- CHN HandiesDocument10 paginiCHN HandiesFreeNursingNotesÎncă nu există evaluări
- The Use of Hypnosis and Systematic Desensitisation in The Management of Dental Phobia A Case ReportDocument6 paginiThe Use of Hypnosis and Systematic Desensitisation in The Management of Dental Phobia A Case ReportAnissa Citra UtamiÎncă nu există evaluări
- Drug Design Metabolism 3Document19 paginiDrug Design Metabolism 3Hanaa HashemÎncă nu există evaluări
- Management of PreeclampsiaDocument11 paginiManagement of PreeclampsiaDanÎncă nu există evaluări
- Mood Disorders Lesson PlanDocument17 paginiMood Disorders Lesson Planapi-2841042060% (1)
- Homeopathy and DentistryDocument3 paginiHomeopathy and DentistrynadiidaÎncă nu există evaluări
- 필라테스 논문Document6 pagini필라테스 논문Kang Hoon KimÎncă nu există evaluări
- Blood Gas Analysis: Zulkifli. DR., Span., Mkes Department of Anesthesiology and Reanimation FK Unsri/ RSMHDocument20 paginiBlood Gas Analysis: Zulkifli. DR., Span., Mkes Department of Anesthesiology and Reanimation FK Unsri/ RSMHIvanRaykaÎncă nu există evaluări
- Approved Practice Setting With Facility License Number and Contact Oct 2023Document30 paginiApproved Practice Setting With Facility License Number and Contact Oct 2023ns5qp4t26dÎncă nu există evaluări
- Critical Care Nursing Diagnosis and Management UrdenDocument8 paginiCritical Care Nursing Diagnosis and Management UrdenMonet0% (1)
- Iliotibial Band Syndrome - FannyDocument13 paginiIliotibial Band Syndrome - FannyAlfiani Rosyida Arisanti Syafi'iÎncă nu există evaluări
- 1-Prirodno Okruzenje I Mentalno ZdravljeDocument8 pagini1-Prirodno Okruzenje I Mentalno ZdravljeUvoBubaÎncă nu există evaluări
- Case Study PresentationDocument21 paginiCase Study Presentationmaeumi3008100% (1)
- A New Neurofeedback Protocol For DepressionDocument12 paginiA New Neurofeedback Protocol For DepressionVezér RóbertÎncă nu există evaluări
- Project Isr - JascapDocument42 paginiProject Isr - JascapPrakrutiShahÎncă nu există evaluări
- Modul 06 PDFDocument16 paginiModul 06 PDFL TereÎncă nu există evaluări
- Application of Orems Theory To NSG PracticeDocument26 paginiApplication of Orems Theory To NSG PracticeLorde Sungcad Ricafrente100% (3)
- Ictus Ortesis MmiiDocument10 paginiIctus Ortesis MmiiCeto Ust Puerto MonttÎncă nu există evaluări
- TB Case Finding (Slide)Document15 paginiTB Case Finding (Slide)Emman Acosta DomingcilÎncă nu există evaluări